Institute of Infection and Global Health, University of Liverpool, Liverpool, UK.
Alder Hey Children's NHS Foundation Trust, Liverpool, UK.
BMJ Qual Saf. 2018 Jul;27(7):521-528. doi: 10.1136/bmjqs-2017-006605. Epub 2017 Sep 29.
To evaluate the impact of integrating a general practitioner (GP) into a tertiary paediatric emergency department (ED) on admissions, waiting times and antibiotic prescriptions.
Retrospective cohort study.
Alder Hey Children's NHS Foundation Trust, a tertiary paediatric hospital in Liverpool, UK.
From October 2014, a GP was colocated within the ED, from 14:00 to 22:00 hours, 7 days a week. Children triaged green on the Manchester Triage System without any comorbidities were classed as 'GP appropriate'. The natural experiment compared patients triaged as 'GP appropriate' and able to be seen by a GP between 14:00 and 22:00 hours (GP group) to patients triaged as 'GP appropriate' seen outside of the hours when a GP was available (ED group). Intention-to-treat (ITT) analysis was used to assess the main outcomes.
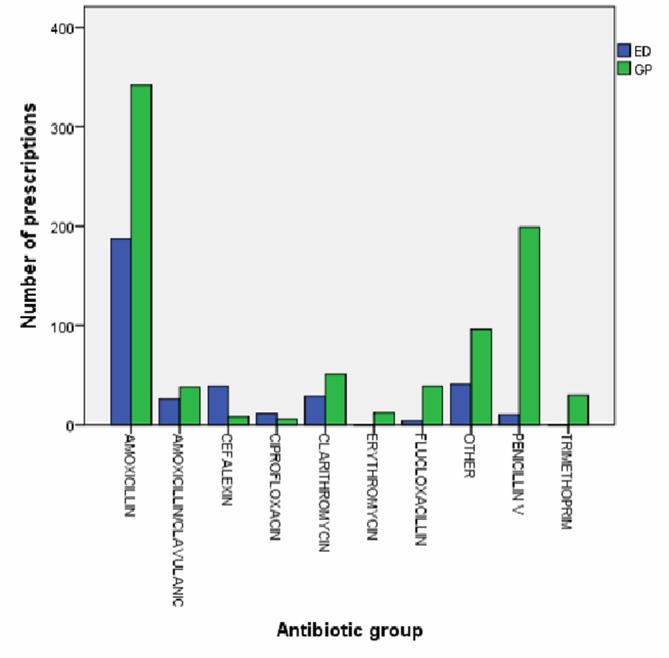
5223 patients were designated as 'GP appropriate'-18.2% of the total attendances to the ED over the study period. There were 2821 (54%) in the GP group and 2402 (46%) in the ED group. The median duration of stay in the ED was 94 min (IQR 63-141) for the GP group compared with 113 min (IQR 70-167) for the ED group (p<0.0005). Using the ITT analysis equivalent, we demonstrated that the GP group were less likely to: be admitted to hospital (2.2% vs 6.5%, OR 0.32, 95% CI 0.24 to 0.44), wait longer than 4 hours (2.3% vs 5.1%, OR 0.45, 95% CI 0.33 to 0.61) or leave before being seen (3.1% vs 5.7%, OR 0.53, 95% CI 0.41 to 0.70), but more likely to receive antibiotics (26.1% vs 20.5%, OR 1.37, 95% CI 1.10 to 1.56). Sensitivity analyses yielded similar results.
Introducing a GP to a paediatric ED service can significantly reduce waiting times and admissions, but may lead to more antibiotic prescribing. This study demonstrates a novel, potentially more efficient ED care pathway in the current context of rising demand for children's emergency services.
评估在三级儿科急诊部(ED)中整合全科医生对入院、等候时间和抗生素处方的影响。
回顾性队列研究。
英国利物浦的奥尔德·希伊儿童国民保健信托基金会,一家三级儿科医院。
自 2014 年 10 月起,一名全科医生每周 7 天,每天 14:00 至 22:00 在 ED 内共同执业。在曼彻斯特分诊系统中分诊为绿色且无合并症的儿童被归类为“适合全科医生”。自然实验将在 14:00 至 22:00 之间能够接受全科医生就诊的分诊为“适合全科医生”的患者(GP 组)与在全科医生可就诊时间之外就诊的分诊为“适合全科医生”的患者(ED 组)进行比较。采用意向治疗(ITT)分析评估主要结局。
在研究期间,共有 5223 名患者被指定为“适合全科医生”——占 ED 总就诊人数的 18.2%。GP 组有 2821 名(54%),ED 组有 2402 名(46%)。GP 组 ED 中位停留时间为 94 分钟(IQR 63-141),而 ED 组为 113 分钟(IQR 70-167)(p<0.0005)。使用 ITT 分析等效方法,我们证明 GP 组不太可能:入院(2.2%比 6.5%,OR 0.32,95%CI 0.24 至 0.44)、等待时间超过 4 小时(2.3%比 5.1%,OR 0.45,95%CI 0.33 至 0.61)或在就诊前离开(3.1%比 5.7%,OR 0.53,95%CI 0.41 至 0.70),但更有可能接受抗生素治疗(26.1%比 20.5%,OR 1.37,95%CI 1.10 至 1.56)。敏感性分析得出了类似的结果。
在儿科 ED 服务中引入全科医生可以显著缩短等候时间和入院时间,但可能会导致更多的抗生素处方。这项研究展示了一种新颖的、潜在更有效的 ED 护理途径,适用于当前儿童急诊服务需求不断增长的情况。