Istituto di Ematologia, Fondazione Policlinico Universitario A Gemelli, Università Cattolica, Roma, Italy
Cattedra di Ematologia, Universita' di Catania, Italy.
Haematologica. 2017 Dec;102(12):2125-2133. doi: 10.3324/haematol.2017.171157. Epub 2017 Sep 29.
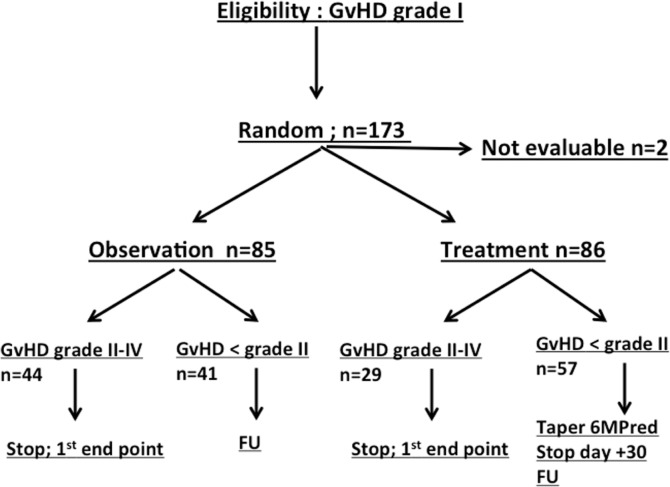
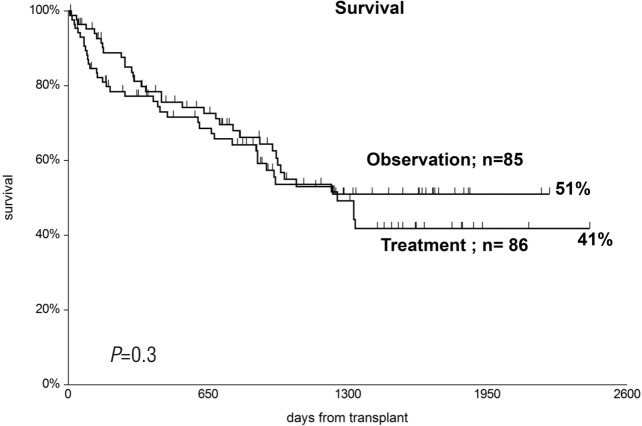
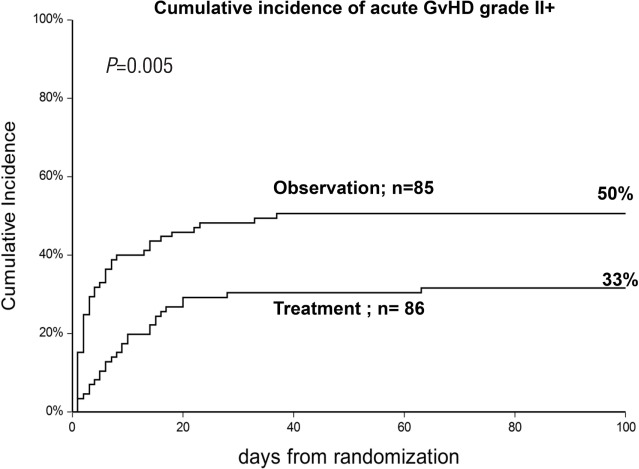
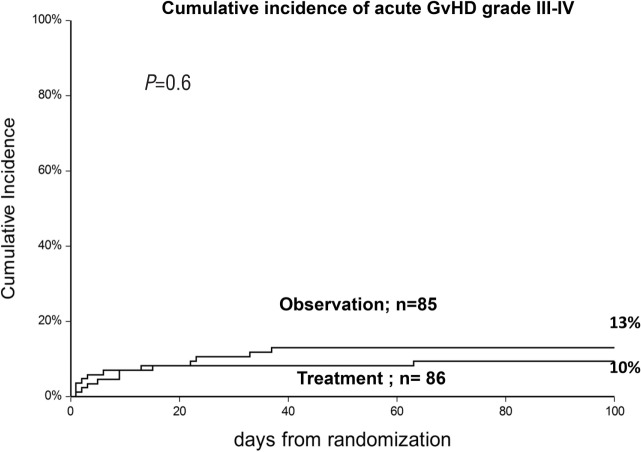
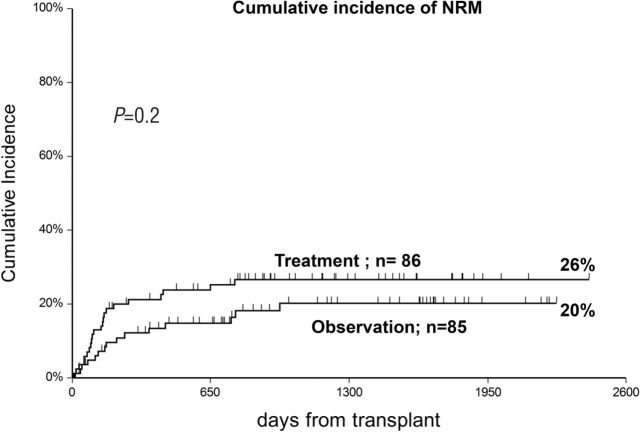
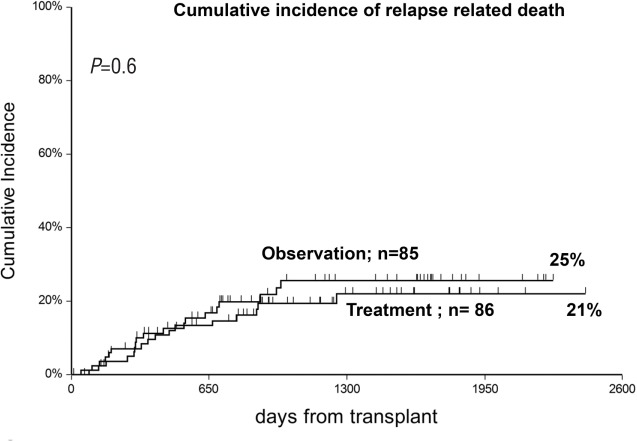
Patients with acute graft--host disease (GvHD) grade I were randomized to an observation arm (n=85) or to a treatment arm (n=86) consisting of 6-methylprednisolone 1 mg/kg/day, after stratification for age and donor type. The primary end point was development of grade II-IV GvHD. The cumulative incidence of grade II-IV GvHD was 50% in the observation arm and 33% in the treatment arm (=0.005). However, grade III-IV GvHD was comparable (13% 10%, respectively; =0.6), and this was true for sibling and alternative donor transplants. Moderate/severe chronic GvHD was also comparable (17% 9%). In multivariate analysis, an early interval between transplant and randomization (<day +20) was the only negative predictor of grade III-IV GvHD. Patients in the observation arm had less infectious bacterial episodes (12 25; =0.04), less severe infectious fungal episodes (0 3; =0.04), and less severe adverse events (3 11; =0.07). At five years, non-relapse mortality was 20% 26% (=0.2), relapse-related mortality 25% 21%, and actuarial survival was 51% 41% (=0.3) in the observation and treatment arms, respectively. In multivariate analysis, advanced disease phase, older age and an early onset of GvHD were significant negative predictors of survival, independent of the randomization arm. In conclusion, steroid treatment of acute grade I GvHD prevents progression to grade II but not to grade III-IV GvHD, and there is no effect on non-relapse mortality and survival. Patients treated with steroids are at a higher risk of developing infections and have more adverse events. ().
患有急性移植物抗宿主病(GVHD)I 级的患者被随机分配到观察组(n=85)或治疗组(n=86),其中观察组接受 1mg/kg/天的 6-甲基泼尼松龙治疗,治疗组在年龄和供体类型方面进行分层。主要终点是发展为 II-IV 级 GVHD。观察组 II-IV 级 GVHD 的累积发生率为 50%,治疗组为 33%(=0.005)。然而,III-IV 级 GVHD 相似(分别为 13%和 10%;=0.6),并且在同胞和替代供体移植中也是如此。中度/重度慢性 GVHD 也相似(分别为 17%和 9%)。多变量分析表明,移植后和随机分组之间的早期时间间隔(<第+20 天)是 III-IV 级 GVHD 的唯一负预测因素。观察组患者发生细菌性感染事件较少(12 例 25 例;=0.04),严重真菌感染事件较少(0 例 3 例;=0.04),严重不良事件较少(3 例 11 例;=0.07)。在五年时,观察组和治疗组的非复发死亡率分别为 20%和 26%(=0.2),复发相关死亡率分别为 25%和 21%,生存率分别为 51%和 41%(=0.3)。多变量分析表明,疾病晚期、年龄较大和 GVHD 早期发生是生存的显著负预测因素,与随机分组无关。总之,急性 I 级 GVHD 的类固醇治疗可防止进展为 II 级,但不能防止进展为 III-IV 级 GVHD,并且对非复发死亡率和生存率没有影响。接受类固醇治疗的患者发生感染和出现更多不良事件的风险更高。()。