Fujimoto Kazuhiro, Kanchiku Tsukasa, Imajo Yasuaki, Suzuki Hidenori, Nishida Norihiro, Funaba Masahiro, Taguchi Toshihiko
Department of Orthopaedic Surgery, Yamaguchi University Graduate School of Medicine, 1-1-1 Minami Kogushi, Ube, Yamaguchi, 755-8505, Japan.
J Orthop Surg Res. 2017 Oct 3;12(1):145. doi: 10.1186/s13018-017-0649-1.
The presence of vertebral fractures affect variations in the termination level of conus medullaris (TLCM) and alter neurological findings. However, few studies have examined association between vertebral fractures, TLCM, and neurological findings. Thus, we herein studied the number and severity of vertebral fractures, TLCM, and neurological findings to clarify the mechanism of neurological deterioration in patients with vertebral fractures.
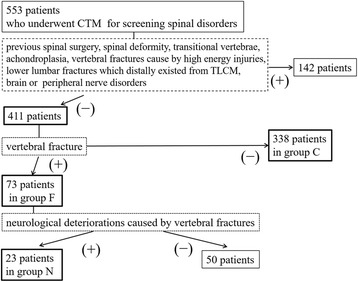
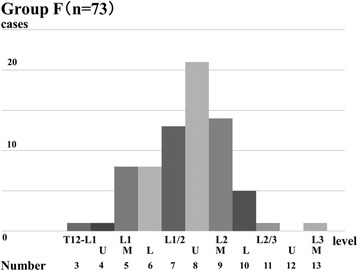
A total of 411 patients who underwent computed tomographic myelography were classified into those with (group F, n = 73) and those without vertebral fractures (group C, n = 338). We assessed correlations between TLCM and age, height, and gender in group C, differences in TLCM between groups F and C, and correlations between TLCM, and the number and severity score of fractures. Neurological evaluations were performed for the patellar tendon reflex (PTR), muscle weakness, sensory disturbance, and bladder contraction disorders.
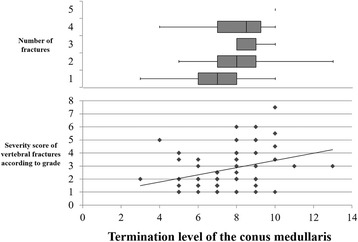
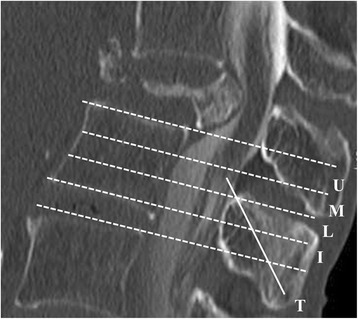
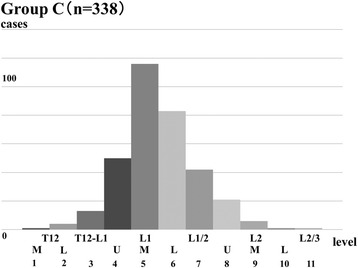
TLCM was most commonly located at the L1 vertebral body in group C and did not significantly differ with age, height, or gender. TLCM was most commonly located at L2 vertebral body in group F. TLCM was more caudally located in group F (P < 0.01). Additionally, there was a significant difference between TLCM and number of fractures, and the severity score of fractures (both P < 0.01). Twenty-three patients showed neurological deterioration by vertebral fractures. Some patients with T12 vertebral fracture showed hyperreflexia of PTR. Serious bladder contraction disorders were seen in patients with compression at close range of TLCM.
We confirmed that vertebral fractures altered location of the TLCM, thus altering potential neurological symptoms. Moreover, there were correlations of the TLCM with the number and severity score of vertebral fractures. Spine surgeons should be cognizant of the relationship between TLCM, level of compressive lesion, and neurological findings to avoid the wrong level in spine surgery and unexpected neurological deteriorations after surgery.
椎体骨折的存在会影响脊髓圆锥终止水平(TLCM)的变化并改变神经学表现。然而,很少有研究探讨椎体骨折、TLCM和神经学表现之间的关联。因此,我们在此研究椎体骨折的数量和严重程度、TLCM以及神经学表现,以阐明椎体骨折患者神经功能恶化的机制。
总共411例行计算机断层脊髓造影的患者被分为有椎体骨折组(F组,n = 73)和无椎体骨折组(C组,n = 338)。我们评估了C组中TLCM与年龄、身高和性别的相关性,F组和C组之间TLCM的差异,以及TLCM与骨折数量和严重程度评分之间的相关性。对髌腱反射(PTR)、肌肉无力、感觉障碍和膀胱收缩障碍进行了神经学评估。
C组中TLCM最常见于L1椎体,且与年龄、身高或性别无显著差异。F组中TLCM最常见于L2椎体。F组中TLCM的位置更靠尾侧(P < 0.01)。此外,TLCM与骨折数量和骨折严重程度评分之间存在显著差异(均P < 0.01)。23例患者因椎体骨折出现神经功能恶化。一些T12椎体骨折的患者表现出PTR亢进。在TLCM近距离受压的患者中可见严重的膀胱收缩障碍。
我们证实椎体骨折改变了TLCM的位置,从而改变了潜在的神经症状。此外,TLCM与椎体骨折的数量和严重程度评分之间存在相关性。脊柱外科医生应认识到TLCM、受压病变水平和神经学表现之间的关系,以避免脊柱手术中定位错误和术后意外的神经功能恶化。