Navarria Pierina, Pessina Federico, Tomatis Stefano, Soffietti Riccardo, Grimaldi Marco, Lopci Egesta, Chiti Arturo, Leonetti Antonella, Casarotti Alessandra, Rossi Marco, Cozzi Luca, Ascolese Anna Maria, Simonelli Matteo, Marcheselli Simona, Santoro Armando, Clerici Elena, Bello Lorenzo, Scorsetti Marta
Radiotherapy and Radiosurgery Department, Humanitas Cancer Center and Research Hospital, Rozzano, Italy.
Neurosurgical Oncology Department, Humanitas Cancer Center and Research Hospital, Rozzano, Italy.
Oncotarget. 2017 Jun 28;8(40):67696-67708. doi: 10.18632/oncotarget.18809. eCollection 2017 Sep 15.
The current standard of care for newly diagnosed glioblastoma (GBM) is surgical resection, followed by radiation therapy (RT) with concurrent and adjuvant temozolomide chemotherapy (TMZ-CHT). The patients outcome is still poor. In this study we evaluated hypofractionated radiation therapy (HFRT), instead of standard fractionated radiation therapy, with concomitant and adjuvant TMZ chemotherapy, in terms of safety and effectiveness.
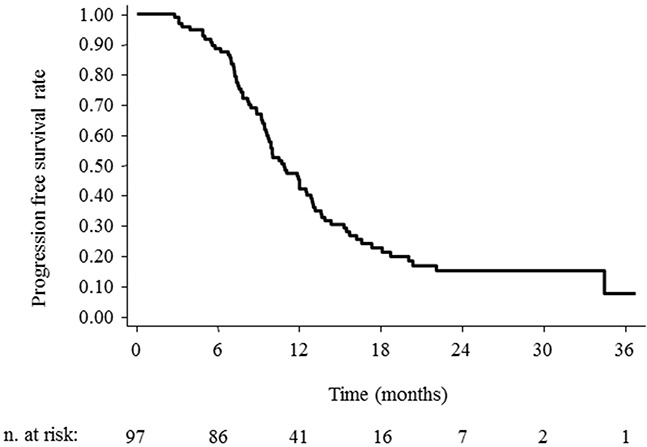
Patients with newly diagnosed GBM, Karnofsky performance scale (KPS) ≥70, and tumor up to 10 cm underwent maximal feasible surgical resection were treated. HFRT consisted of 60 Gy, in daily fractions of 4 Gy given 5 days per week for 3 weeks. The primary endpoints were overall survival (OS), progression free survival (PFS), and incidence of radiation induced brain toxicity. Secondary endpoint was the evaluation of neurocognitive function.
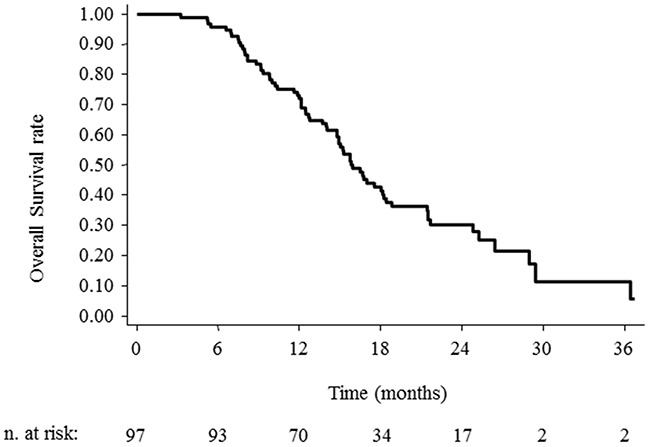
A total of 97 patients were included in this phase II study. The median age was 60.5 years (range 23-77 years). Debulking surgery was performed in 83.5% of patients, HFRT was completed in all 97 patients, concurrent and adjuvant TMZ in 93 (95.9%). The median number of TMZ cycles was six (range 1-12 cycles). No severe toxicity occurred and the neuropsychological evaluation remained stable. At a median follow up time of 15.2 months the median OS time, 1,2-year OS rate were 15.9 months (95% CI 14-18), 72.2% (95% CI 62.1-80) and 30.4% (95% CI 20.8-40.6). Age, KPS, MGMT methylation status, and extent of surgical resection were significant factors influencing the outcome.
HFRT with concomitant and adjuvant TMZ chemotherapy is an effective and safe treatment.
新诊断的胶质母细胞瘤(GBM)目前的标准治疗方案是手术切除,随后进行放射治疗(RT)并同步及辅助替莫唑胺化疗(TMZ-CHT)。患者的预后仍然很差。在本研究中,我们评估了超分割放射治疗(HFRT)联合辅助TMZ化疗,而非标准分割放射治疗,在安全性和有效性方面的情况。
对新诊断的GBM患者进行治疗,这些患者卡氏功能状态评分(KPS)≥70,肿瘤最大直径达10 cm,接受了最大程度可行的手术切除。HFRT总剂量为60 Gy,每周5天,每天4 Gy,共3周。主要终点为总生存期(OS)、无进展生存期(PFS)和放射性脑毒性的发生率。次要终点是神经认知功能的评估。
共有97例患者纳入了这项II期研究。中位年龄为60.5岁(范围23 - 77岁)。83.5%的患者进行了肿瘤大部切除术,97例患者均完成了HFRT,93例(95.9%)患者接受了同步及辅助TMZ化疗。TMZ化疗的中位周期数为6个(范围1 - 12个周期)。未发生严重毒性反应,神经心理学评估结果保持稳定。中位随访时间为15.2个月时,中位OS时间、1年和2年OS率分别为15.9个月(95%CI 14 - 18)、72.2%(95%CI 62.1 - 80)和30.4%(95%CI 20.8 - 40.6)。年龄、KPS、MGMT甲基化状态和手术切除范围是影响预后的重要因素。
HFRT联合辅助TMZ化疗是一种有效且安全的治疗方法。