Allinovi Marco, Cirami Calogero Lino, Caroti Leonardo, Antognoli Giulia, Farsetti Silvia, Amato Maria Pia, Minetti Enrico Eugenio
Nephrology Unit, Careggi University Hospital, Florence, Italy.
Department of NEUROFARBA, Section Neuroscience, University of Florence, Florence, Italy.
Clin Kidney J. 2017 Oct;10(5):625-631. doi: 10.1093/ckj/sfw143. Epub 2017 Feb 16.
Interferon-beta (IFN-beta) is one of the most widely prescribed medications for relapsing-remitting multiple sclerosis (RRMS). IFN-related thrombotic microangiopathy (TMA) is a rare but severe complication, with a fulminant clinical onset and a possibly life-threatening outcome that may occur years after a well-tolerated treatment with IFN. Most patients evolve rapidly to advanced chronic kidney disease and eventually to renal failure.
We performed a retrospective analysis of TMA cases diagnosed and managed in our Nephrology Department from 2010 to 2015, and performed a literature review of IFN-beta-induced TMA.
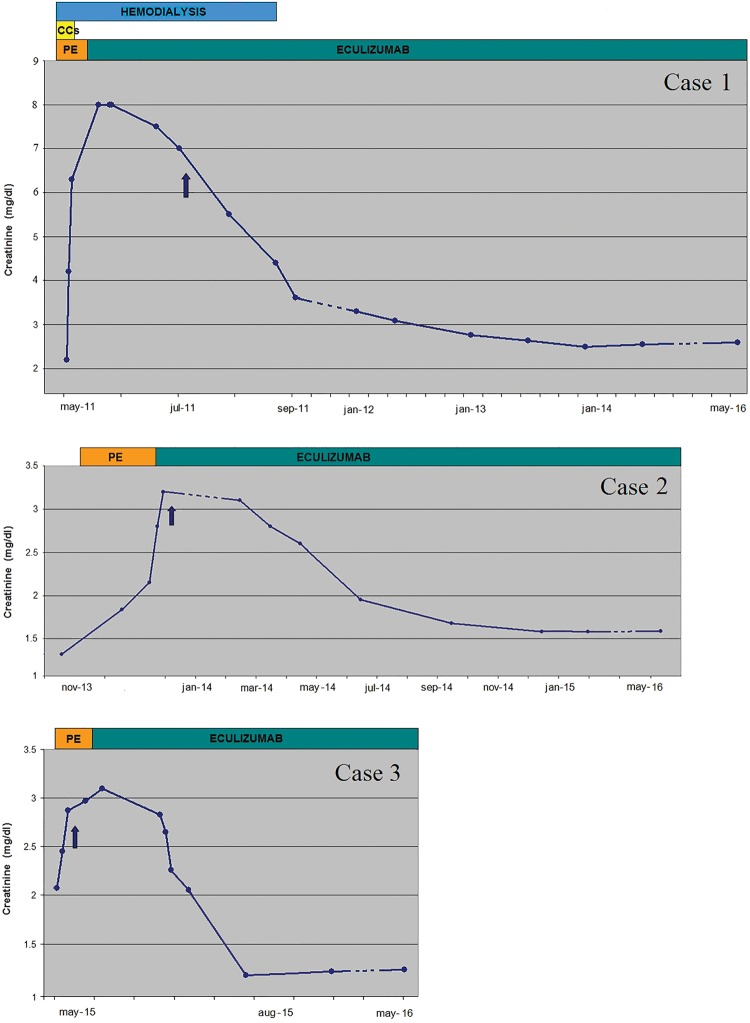
Three cases of TMA among patients treated with IFN-beta were identified who did not show any renal improvement following conventional therapy: IFN withdrawal and plasma exchange (PE, range 8-18) sessions. All of them responded favourably to eculizumab, with progressive clinical and renal improvement, allowing dialysis discontinuation, without recurrence of TMA during a long-term follow-up (range 1-5 years).
TMA is a recognized severe complication in RRMS patients treated with IFN-beta. Withdrawal of IFN and treatment with PE, steroids or rituximab did not improve the poor renal prognosis in our three patients and in all the previously described cases in the literature. In our experience, eculizumab had a strikingly favourable effect on renal recovery, suggesting a role of IFN-beta as a trigger in complement-mediated TMA. Neurologists and nephrologists should be vigilant to this complication to prevent possibly irreversible renal damage.
β-干扰素(IFN-β)是复发缓解型多发性硬化症(RRMS)最常用的处方药之一。IFN相关血栓性微血管病(TMA)是一种罕见但严重的并发症,临床起病急骤,可能危及生命,可发生于对IFN耐受良好的治疗数年之后。大多数患者会迅速发展为晚期慢性肾脏病,最终发展为肾衰竭。
我们对2010年至2015年在我们肾脏病科诊断和处理的TMA病例进行了回顾性分析,并对IFN-β诱导的TMA进行了文献综述。
在接受IFN-β治疗的患者中,发现了3例TMA病例,这些患者在接受常规治疗(停用IFN和进行血浆置换(PE,8 - 18次))后肾脏情况未改善。所有患者对依库珠单抗反应良好,临床和肾脏情况逐渐改善,可停止透析,在长期随访(1 - 5年)期间TMA未复发。
TMA是接受IFN-β治疗的RRMS患者中公认的严重并发症。停用IFN以及使用PE、类固醇或利妥昔单抗治疗,并未改善我们3例患者以及文献中所有先前描述病例的不良肾脏预后。根据我们的经验,依库珠单抗对肾脏恢复有显著的良好效果,提示IFN-β在补体介导的TMA中起触发作用。神经科医生和肾脏科医生应警惕这种并发症,以防止可能出现的不可逆肾脏损害。