National Laboratory for Scientific Computing, Petrópolis, Brazil.
National Institute of Science and Technology in Medicine Assisted by Scientific Computing, INCT-MACC, Petrópolis, Brazil.
Stroke Vasc Neurol. 2017 Jun 8;2(3):108-117. doi: 10.1136/svn-2017-000087. eCollection 2017 Sep.
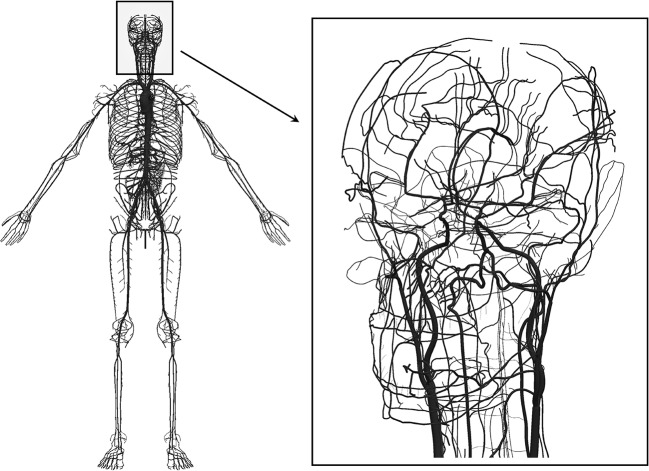
The role of hypertension in cerebral small vessel disease is poorly understood. At the base of the brain (the 'vascular centrencephalon'), short straight arteries transmit blood pressure directly to small resistance vessels; the cerebral convexity is supplied by long arteries with many branches, resulting in a drop in blood pressure. Hypertensive small vessel disease (lipohyalinosis) causes the classically described lacunar infarctions at the base of the brain; however, periventricular white matter intensities (WMIs) seen on MRI and WMI in subcortical areas over the convexity, which are often also called 'lacunes', probably have different aetiologies.
We studied pressure gradients from proximal to distal regions of the cerebral vasculature by mathematical modelling.
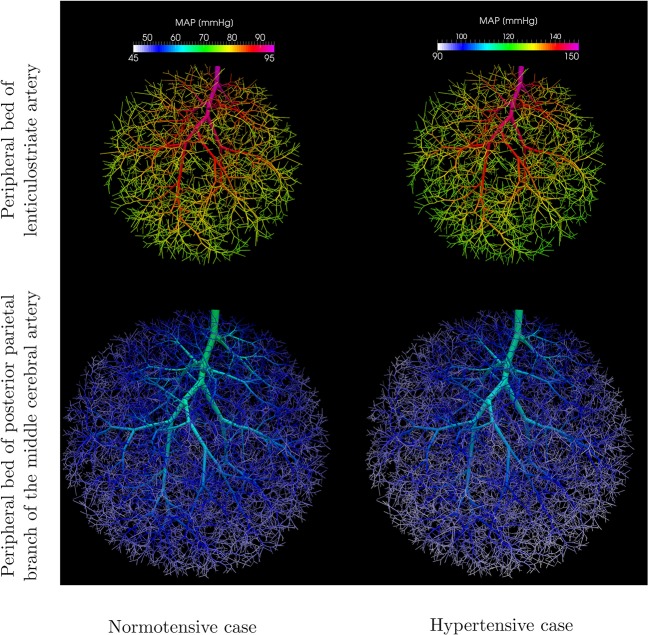
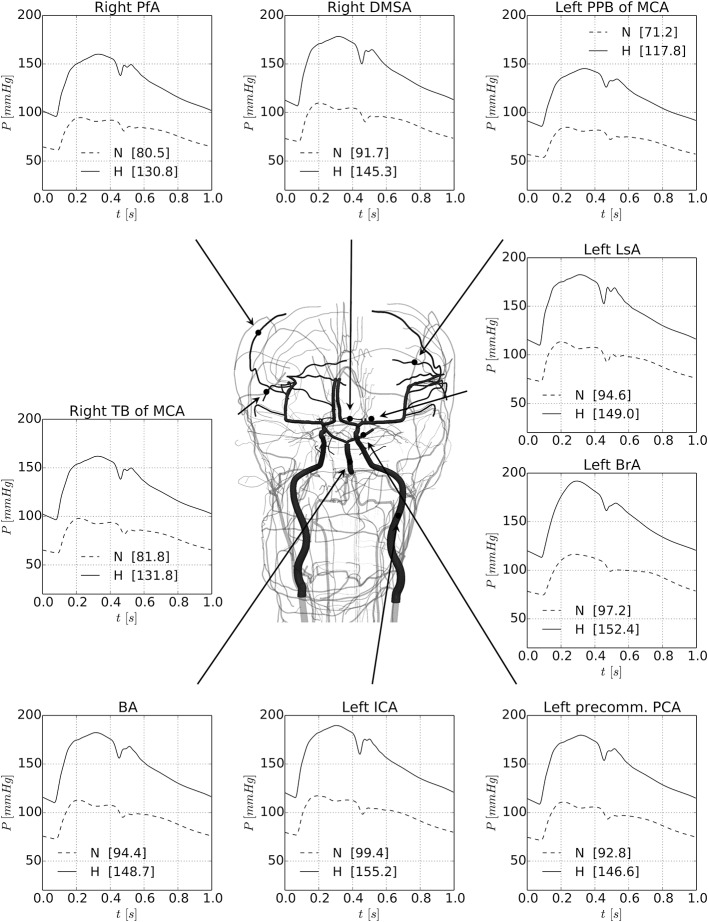
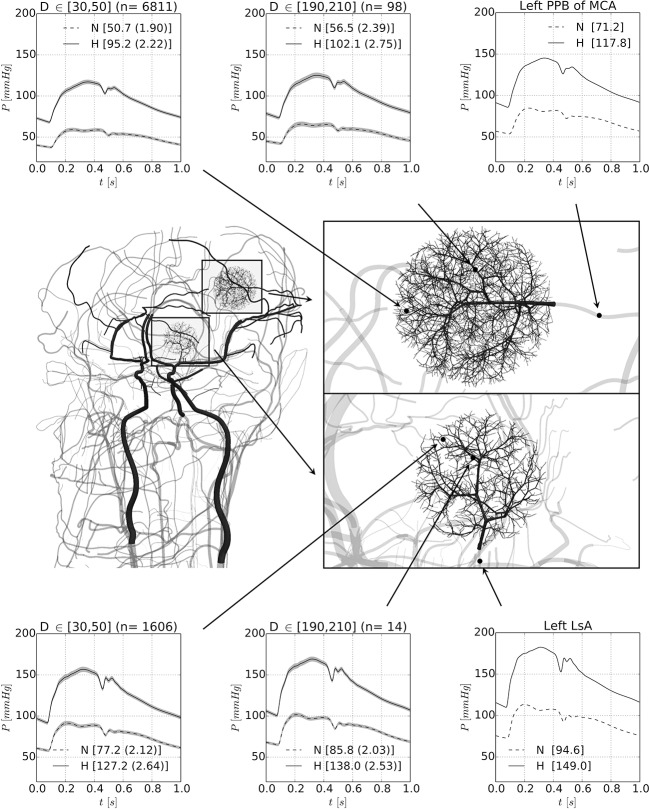
Blood flow/pressure equations were solved in an Anatomically Detailed Arterial Network (ADAN) model, considering a normotensive and a hypertensive case. Model parameters were suitably modified to account for structural changes in arterial vessels in the hypertensive scenario. Computations predict a marked drop in blood pressure from large and medium-sized cerebral vessels to cerebral peripheral beds. When blood pressure in the brachial artery is 192/113 mm Hg, the pressure in the small arterioles of the posterior parietal artery bed would be only 117/68 mm Hg. In the normotensive case, with blood pressure in the brachial artery of 117/75 mm Hg, the pressure in small parietal arterioles would be only 59/38 mm Hg.
These findings have important implications for understanding small vessel disease. The marked pressure gradient across cerebral arteries should be taken into account when evaluating the pathogenesis of small WMIs on MRI. Hypertensive small vessel disease, affecting the arterioles at the base of the brain should be distinguished from small vessel disease in subcortical regions of the convexity and venous disease in the periventricular white matter.
高血压在脑小血管疾病中的作用尚不清楚。在脑底部(“血管中央脑”),短直动脉将血压直接传递给小阻力血管;大脑凸面由具有许多分支的长动脉供应,导致血压下降。高血压小血管病(脂质透明变性)导致基底节区典型的腔隙性梗死;然而,MRI 上见到的脑室周围白质强度(WMIs)和凸面皮质下区域的 WMIs 通常也称为“腔隙”,可能具有不同的病因。
通过数学建模研究脑血管从近端到远端区域的压力梯度。
在考虑正常血压和高血压病例的情况下,我们在解剖详细的动脉网络(ADAN)模型中求解了血流/压力方程。模型参数进行了适当修改,以考虑高血压情况下动脉血管的结构变化。计算预测,从大、中动脉到脑周围床,血压会显著下降。当肱动脉血压为 192/113mmHg 时,后顶叶动脉床小动脉的血压仅为 117/68mmHg。在正常血压病例中,肱动脉血压为 117/75mmHg,小顶叶动脉的血压仅为 59/38mmHg。
这些发现对理解小血管疾病具有重要意义。在评估 MRI 上小 WMIs 的发病机制时,应考虑到脑动脉的明显压力梯度。影响脑底部小动脉的高血压小血管病应与凸面皮质下区域的小血管病和脑室周围白质的静脉病区分开来。