Division of Nephrology and Hypertension, Mayo Clinic, Rochester, MN 55902, USA.
European University of Western Brittany, CHU Brest, Brest, France.
Nephrol Dial Transplant. 2018 Apr 1;33(4):645-652. doi: 10.1093/ndt/gfx188.
The PROPKD score has been proposed to stratify the risk of progression to end-stage renal disease in autosomal dominant polycystic kidney disease (ADPKD) subjects. We aimed to assess its prognostic value in a genotyped subgroup of subjects from the Tolvaptan Phase 3 Efficacy and Safety Study in Autosomal Dominant Polycystic Kidney Disease (TEMPO3/4) trial.
In the post hoc analysis, PKD1 and PKD2 were screened in 770 subjects and the PROPKD score was calculated in mutation-positive subjects (male: 1 point; hypertension <35 years: 2 points; first urologic event <35 years: 2 points; nontruncating PKD1 mutation: 2 points; truncating PKD1 mutation: 4 points). Subjects were classified into low-risk (LR; 0-3 points), intermediate-risk (IR; 4-6 points) and high-risk (HR; 7-9 points) groups.
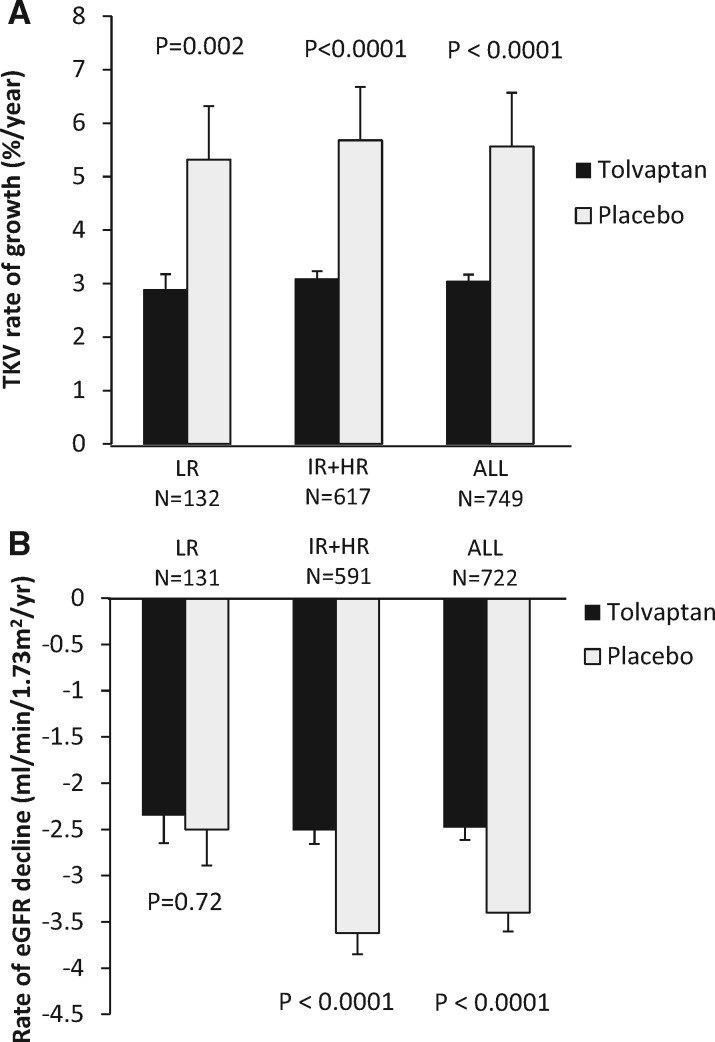
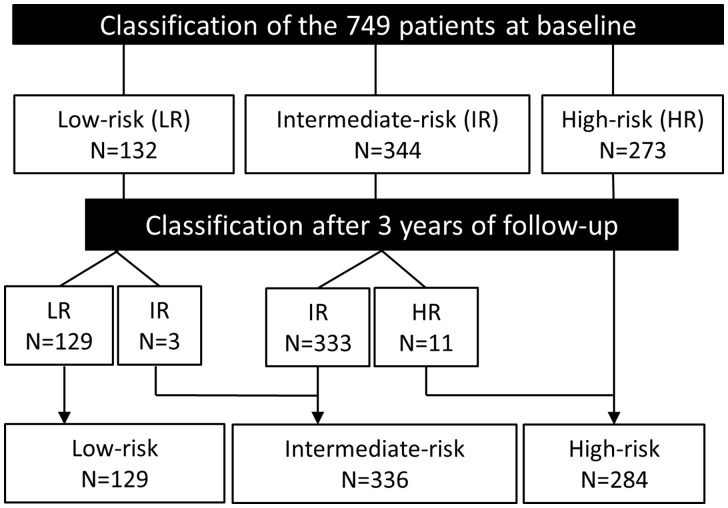
The PROPKD score was calculated in 749 subjects (LR = 132, IR = 344 and HR = 273); age was inversely related to risk (LR = 43.6 years, IR = 39.5 years, HR = 36.2 years; P < 0.001). Subjects from the HR group had significantly higher height-adjusted total kidney volume (TKV) and rates of TKV growth. While baseline renal function was similar across all risk groups, the rate of estimated glomerular filtration rate (eGFR) decline significantly increased from LR to HR in the placebo group. Tolvaptan treatment effectiveness to reduce TKV growth was similar in all three risk categories. While tolvaptan significantly slowed eGFR decline in the IR (tolvaptan = -2.34 versus placebo = -3.33 mL/min/1.73 m2/year; P = 0.008) and HR groups (tolvaptan = -2.74 versus placebo = -3.94 mL/min/1.73 m2/year; P = 0.002), there was no difference in the LR group (tolvaptan = -2.35 versus placebo = -2.50 mL/min/1.73 m2/year; P = 0.72). Excluding the LR subjects from the analysis improved the apparent treatment effect of tolvaptan on eGFR decline.
This study confirms the prognostic value of the PROPKD score and suggests that it could reduce costs and enhance endpoint sensitivity by enriching future study populations for rapidly progressing ADPKD subjects.
PROPKD 评分被提议用于分层常染色体显性遗传多囊肾病(ADPKD)患者进展为终末期肾病的风险。我们旨在评估其在 Tolvaptan 三期疗效和安全性研究中常染色体显性遗传多囊肾病(TEMPO3/4)试验的基因分型亚组中的预后价值。
在事后分析中,对 770 例患者进行了 PKD1 和 PKD2 筛查,并计算了突变阳性患者的 PROPKD 评分(男性:1 分;高血压<35 岁:2 分;首次泌尿科事件<35 岁:2 分;非截断 PKD1 突变:2 分;截断 PKD1 突变:4 分)。将患者分为低危(LR;0-3 分)、中危(IR;4-6 分)和高危(HR;7-9 分)组。
在 749 例患者中计算了 PROPKD 评分(LR=132,IR=344,HR=273);年龄与风险呈负相关(LR=43.6 岁,IR=39.5 岁,HR=36.2 岁;P<0.001)。高危组患者的身高调整后总肾体积(TKV)和 TKV 增长率明显更高。虽然所有风险组的基线肾功能相似,但在安慰剂组中,估算肾小球滤过率(eGFR)下降的速度从 LR 显著增加到 HR。托伐普坦治疗降低 TKV 生长的效果在所有三个风险类别中相似。虽然托伐普坦在 IR 组(托伐普坦=-2.34 与安慰剂=-3.33mL/min/1.73m2/年;P=0.008)和 HR 组(托伐普坦=-2.74 与安慰剂=-3.94mL/min/1.73m2/年;P=0.002)中显著减缓 eGFR 下降,但在 LR 组中没有差异(托伐普坦=-2.35 与安慰剂=-2.50mL/min/1.73m2/年;P=0.72)。从分析中排除 LR 患者,提高了托伐普坦对 eGFR 下降的治疗效果。
本研究证实了 PROPKD 评分的预后价值,并表明它可以通过富集快速进展性 ADPKD 患者的未来研究人群来降低成本并提高终点敏感性。