National Heart and Lung Institute, Imperial College, Dovehouse Street, London, UK.
Division of Cardiology, Department of Internal Medicine II, University Hospital Regensburg, Franz-Josef-Strauß-Allee 11, Regensburg, Germany.
Europace. 2018 Aug 1;20(8):1352-1361. doi: 10.1093/europace/eux246.
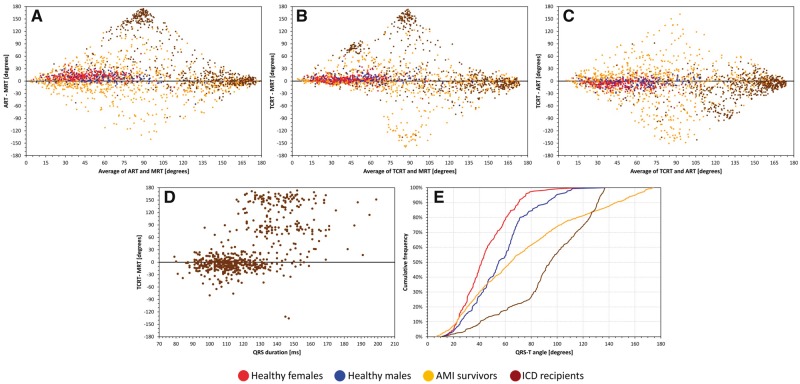
Increased spatial angle between QRS complex and T wave loop orientations has repeatedly been shown to predict cardiac risk. However, there is no consensus on the methods for the calculation of the angle. This study compared the reproducibility and predictive power of three most common ways of QRS-T angle assessment.
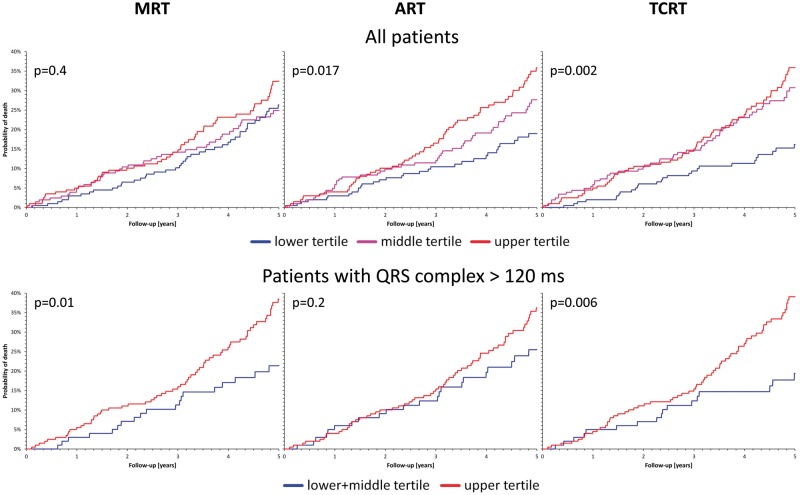
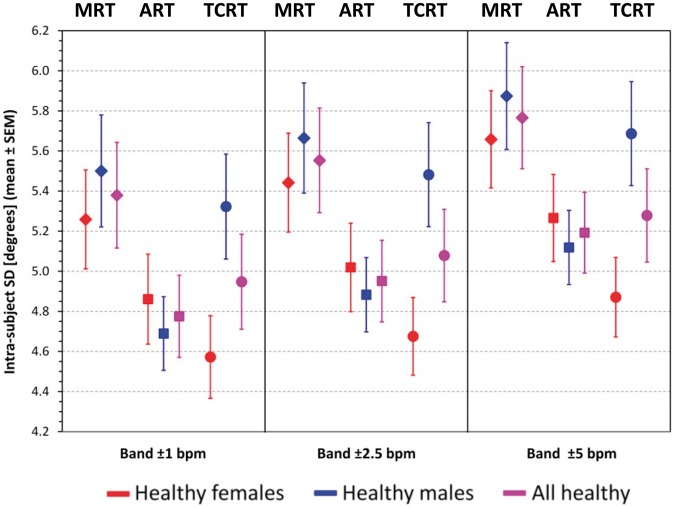
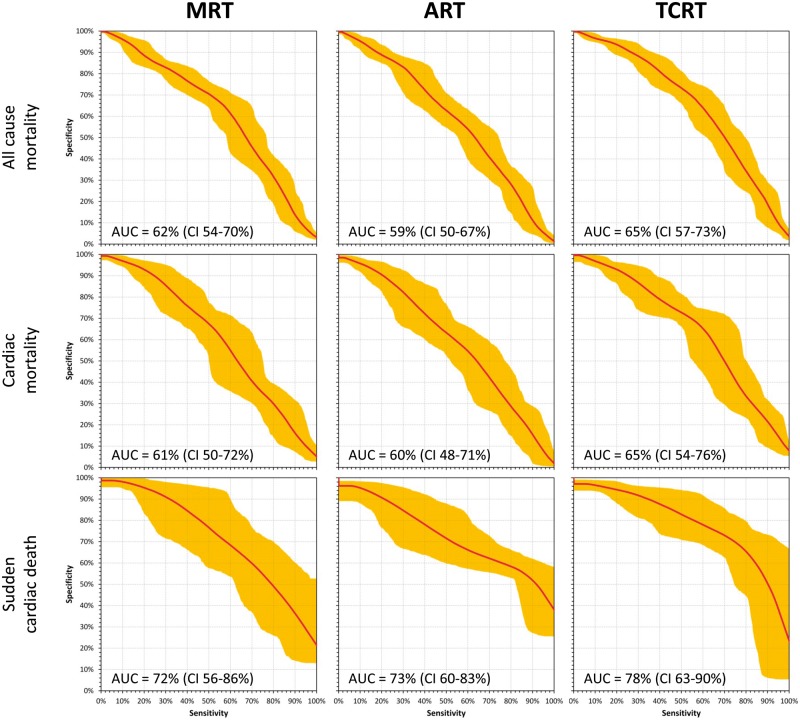
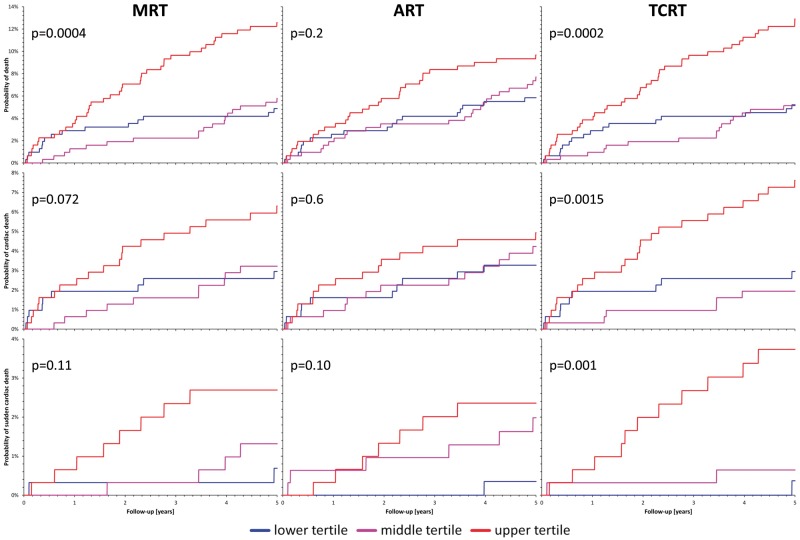
Electrocardiograms of 352 healthy subjects, 941 survivors of acute myocardial infarction (MI), and 605 patients recorded prior to the implantation of automatic defibrillator [implantable cardioverter defibrillator (ICD)] were used to obtain QRS-T angle measurements by the maximum R to T (MRT), area R to T (ART), and total cosine R to T (TCRT) methods. The results were compared in terms of physiologic reproducibility and power to predict mortality in the cardiac patients during 5-year follow-up. Maximum R to T results were significantly less reproducible compared to the other two methods. Among both survivors of acute MI and ICD recipients, TCRT method was statistically significantly more powerful in predicting mortality during follow-up. Among the acute MI survivors, increased spatial QRS-T angle (TCRT assessment) was particularly powerful in predicting sudden cardiac death with the area under the receiver operator characteristic of 78% (90% confidence interval 63-90%). Among the ICD recipients, TCRT also predicted mortality significantly among patients with prolonged QRS complex duration when the spatial orientation of the QRS complex is poorly defined.
The TCRT method for the assessment of spatial QRS-T angle appears to offer important advantages in comparison to other methods of measurement. This approach should be included in future clinical studies of the QRS-T angle. The TCRT method might also be a reasonable candidate for the standardization of the QRS-T angle assessment.
QRS 复合波与 T 波环方向之间的空间夹角增加已被反复证明可预测心脏风险。然而,对于夹角的计算方法尚未达成共识。本研究比较了三种最常用的 QRS-T 角评估方法的可重复性和预测能力。
使用 352 例健康受试者、941 例急性心肌梗死(MI)幸存者和 605 例在植入自动除颤器(植入式心脏复律除颤器[ICD])之前记录的心电图,通过最大 R 到 T(MRT)、面积 R 到 T(ART)和总余弦 R 到 T(TCRT)方法获得 QRS-T 角测量值。比较了这三种方法在生理可重复性和预测心脏患者 5 年随访期间死亡率方面的能力。与其他两种方法相比,最大 R 到 T 结果的可重复性明显较差。在急性 MI 幸存者和 ICD 接受者中,TCRT 方法在预测随访期间死亡率方面具有统计学意义上的更大优势。在急性 MI 幸存者中,增加的 QRS-T 角(TCRT 评估)在预测心脏性猝死方面特别有效,受试者工作特征曲线下面积为 78%(90%置信区间 63-90%)。在 ICD 接受者中,TCRT 也在 QRS 复合体持续时间延长且 QRS 复合体空间方向定义较差的患者中显著预测死亡率。
与其他测量方法相比,TCRT 评估空间 QRS-T 角的方法似乎具有重要优势。这种方法应该纳入未来 QRS-T 角的临床研究中。TCRT 方法也可能是 QRS-T 角评估标准化的合理候选方法。