Seegers Joachim, Hnatkova Katerina, Friede Tim, Malik Marek, Zabel Markus
Department of Cardiology and Pneumology, Division of Clinical Electrophysiology, University Medical Center Göttingen, Göttingen, Germany.
Department of Internal Medicine II, Division of Cardiology, Section of Electrophysiology, University Hospital Regensburg, Regensburg, Germany.
PLoS One. 2017 Mar 14;12(3):e0173868. doi: 10.1371/journal.pone.0173868. eCollection 2017.
In implantable cardioverter-defibrillator (ICD) patients, predictors of ICD shocks and mortality are needed to improve patient selection. Electrocardiographic (ECG) markers are simple to obtain and have been demonstrated to predict mortality. We aimed to assess the association of T-wave loop area and circularity with ICD shocks.
The study investigated patients with ICDs implanted between 1998 and 2010 for whom digital 12-lead ECGs (Schiller CS200 ECG-Network) of sufficient quality were obtained within 1 month prior to the implantation. T-wave loop area and circularity were calculated. Follow-up data of appropriate shocks were obtained during ICD clinic visits that included reviews of device stored electrograms.
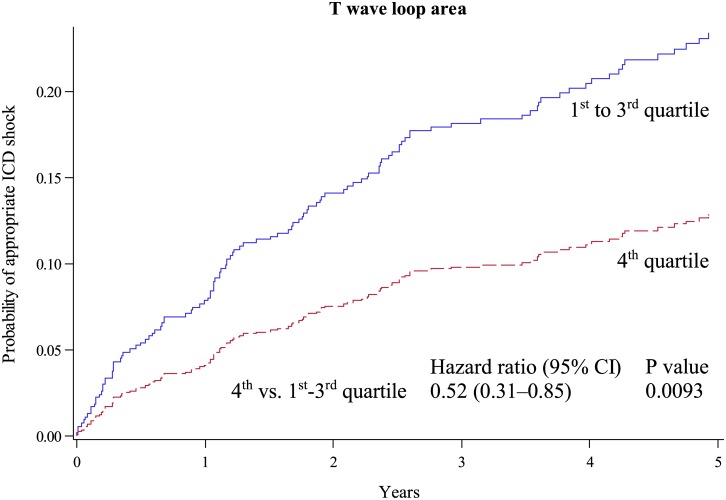
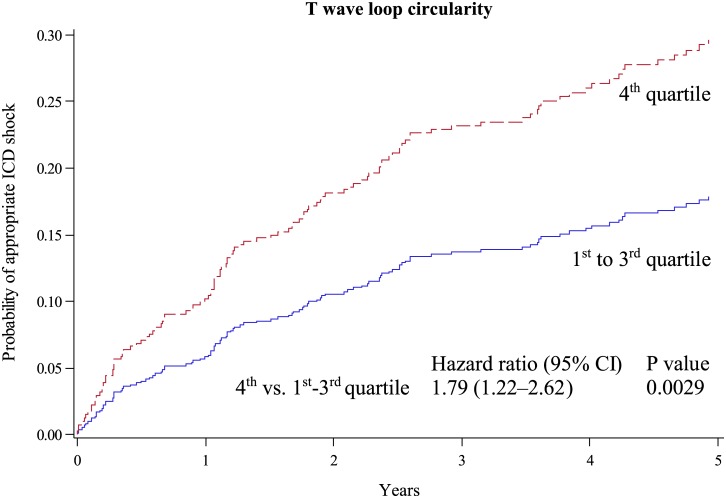
A total of 605 patients (82% males) were included; 68% had ischemic cardiomyopathy and 72% were treated for primary prevention. Over 3.8±1.4 years of follow-up, 114 patients (19%) experienced appropriate shock(s). Those with smaller T-wave loop area received fewer shocks (TLA, hazard ratio, HR, per increase of 1 technical unit, 0.71; [95% confidence interval, 0.53-0.94]; P = 0.02) and those with larger T-wave loop circularity (TLC) representing rounder T wave loop received more shocks (HR per 1% TLC increase 2.96; [0.85-10.36]; P = 0.09). When the quartile containing the largest TLA and TLC values, respectively, were compared to the remaining cases, TLA remained significantly associated with fewer and TLC with more frequent shocks also after multivariate adjustment for clinical variables (HR, 0.59 [0.35-0.99], P = 0.044; and 1.64 [1.08-2.49], P = 0.021, respectively).
The size and shape of the T-wave loop calculated from pre-implantation 12-lead ECGs are associated with appropriate ICD shocks.
在植入式心律转复除颤器(ICD)患者中,需要确定ICD电击和死亡率的预测因素以优化患者选择。心电图(ECG)标志物易于获取且已被证实可预测死亡率。我们旨在评估T波环面积和圆形度与ICD电击的相关性。
本研究调查了1998年至2010年间植入ICD的患者,这些患者在植入前1个月内获得了质量足够的数字化12导联心电图(席勒CS200心电图网络)。计算T波环面积和圆形度。在ICD门诊随访期间获取适当电击的随访数据,其中包括对设备存储的心电信号进行回顾。
共纳入605例患者(82%为男性);68%患有缺血性心肌病,72%接受一级预防治疗。在3.8±1.4年的随访中,114例患者(19%)经历了适当的电击。T波环面积较小的患者接受电击次数较少(TLA,风险比,HR,每增加1个技术单位,0.71;[95%置信区间,0.53 - 0.94];P = 0.02),而T波环圆形度较大(TLC)代表更圆的T波环的患者接受电击次数更多(每增加1%TLC,HR为2.96;[0.85 - 10.36];P = 0.09)。当分别将包含最大TLA和TLC值的四分位数与其余病例进行比较时,在对临床变量进行多因素调整后,TLA仍与较少的电击显著相关,TLC与更频繁的电击显著相关(HR分别为0.59 [0.35 - 0.99],P = 0.044;和1.64 [1.08 - 2.49],P = 0.021)。
植入前12导联心电图计算得出的T波环大小和形状与ICD适当电击相关。