Haque Reina, UlcickasYood Marianne, Xu Xiaoqing, Cassidy-Bushrow Andrea E, Tsai Huei-Ting, Keating Nancy L, Van Den Eeden Stephen K, Potosky Arnold L
Department of Research and Evaluation, Kaiser Permanente Southern California, Pasadena, CA 91101, USA.
Department of Epidemiology, Boston University School of Public Health, Boston, MA 02118, USA.
Br J Cancer. 2017 Oct 10;117(8):1233-1240. doi: 10.1038/bjc.2017.280. Epub 2017 Aug 24.
As androgen deprivation therapy (ADT) is increasingly being used in men with localised prostate cancer, our goal was to examine the association between ADT and the risk of cardiovascular disease (CVD).
We conducted a prospective cohort study using records of a large health-care system in California. The study included men with newly diagnosed localised prostate cancer (1998-2008) who initially underwent active surveillance (N=7637) and were followed through 2010. We examined 10 individual CVD outcomes. Cox proportional hazard models incorporated time-varying treatment variables and controlled for race/ethnicity, age, and tumour characteristics, recurrence risk, CVD medication use, and CVD risk factors.
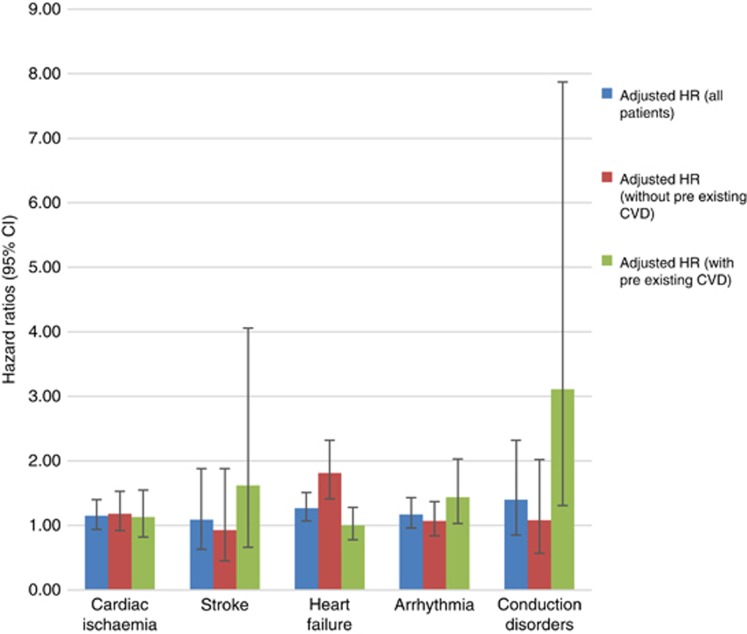
Of the 7637 subjects, nearly 30% were exposed to ADT. In the multivariable analyses, ADT was associated with an increased risk of heart failure (adjusted HR=1.81, 95% CI 1.40-2.32) in men without preexisting CVD. Elevated risks of arrhythmia (adjusted HR=1.44, 95% CI 1.02-2.01), and conduction disorder (adjusted HR=3.11, 95% CI 1.22, 7.91) were only observed among patients with preexisting CVD.
In men with clinically localised prostate cancer who were initially under active surveillance, ADT was associated with a greater risk of heart failure in men without any preexisting CVD. We also found an increased risk of arrhythmia and conduction disorder in men with preexisting CVD. This study provides the basis for identifying high-risk men treated with ADT who might benefit from regular cardiac monitoring and lifestyle modification recommendations.
随着雄激素剥夺疗法(ADT)越来越多地用于局部前列腺癌男性患者,我们的目标是研究ADT与心血管疾病(CVD)风险之间的关联。
我们利用加利福尼亚一个大型医疗保健系统的记录进行了一项前瞻性队列研究。该研究纳入了新诊断为局部前列腺癌(1998 - 2008年)且最初接受主动监测的男性患者(N = 7637),并随访至2010年。我们研究了10种个体心血管疾病结局。Cox比例风险模型纳入了随时间变化的治疗变量,并对种族/民族、年龄、肿瘤特征、复发风险、心血管疾病药物使用情况和心血管疾病风险因素进行了控制。
在7637名受试者中,近30%接受了ADT治疗。在多变量分析中,对于既往无心血管疾病的男性,ADT与心力衰竭风险增加相关(校正后风险比[HR] = 1.81,95%置信区间[CI] 1.40 - 2.32)。仅在既往有心血管疾病的患者中观察到心律失常风险升高(校正后HR = 1.44,95% CI 1.02 - 2.01)和传导障碍风险升高(校正后HR = 3.11,95% CI 1.22,7.91)。
在最初接受主动监测的临床局部前列腺癌男性患者中,ADT与既往无任何心血管疾病的男性发生心力衰竭的风险更高相关。我们还发现既往有心血管疾病的男性发生心律失常和传导障碍的风险增加。本研究为识别接受ADT治疗的高危男性提供了依据,这些男性可能受益于定期心脏监测和生活方式改变建议。