Lee Seung Hyun, Chang Byung Chul, Youn Young-Nam, Joo Hyun Chel, Yoo Kyung-Jong, Lee Sak
Division of Thoracic and Cardiovascular Surgery, Severance Cardiovascular Hospital, Yonsei Cardiovascular Research Institute, Yonsei University, College of Medicine, 250 Seongsanno, Seodaemun-gu, Seoul, 03722, Republic of Korea.
J Cardiothorac Surg. 2017 Oct 10;12(1):88. doi: 10.1186/s13019-017-0653-x.
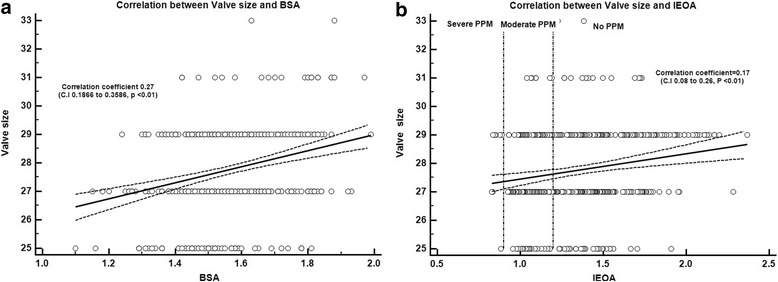
Prosthesis-patient mismatch (PPM) is characterised by the effects of inadequate prosthesis size relative to body surface area (BSA).The purpose of this study was to determine the impact of PPM on late clinical outcomes after mitral valve replacement (MVR) in rheumatic population.
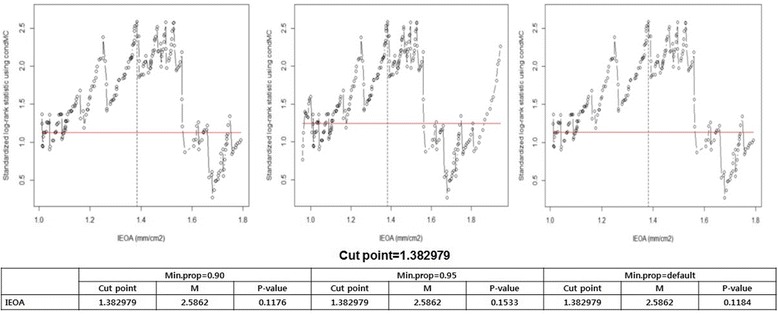
From 2000 to 2013, a total of 445 patients (mean age 54.2 ± 11.7 years) underwent isolated MVR (±tricuspid annuloplasty) for rheumatic disease were investigated. Effective orifice area (EOA) was determined by the continuity equation and PPM was defined as indexed EOA (EOA/BSA) ≤ 1.2 cm/m. Clinical and echocardiographic follow-up (mean follow up 8.7 ± 4.0 years) results were compared.
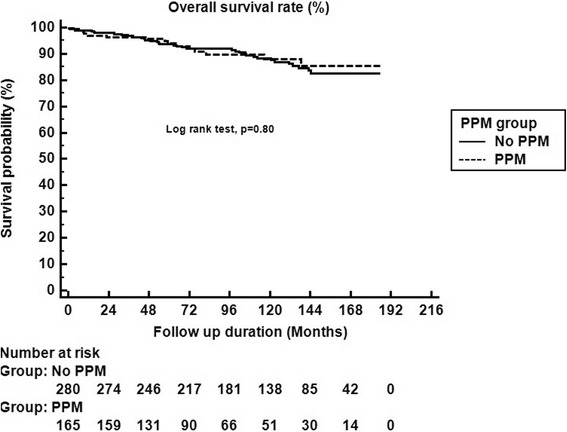
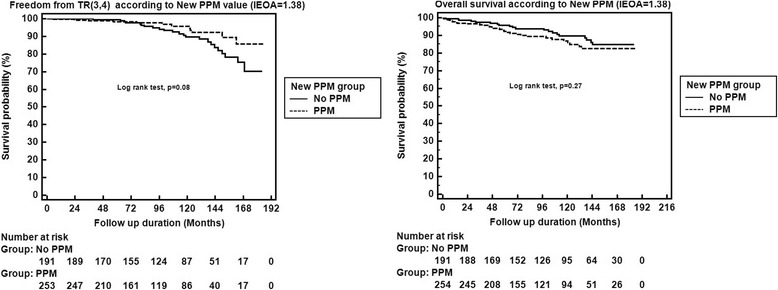
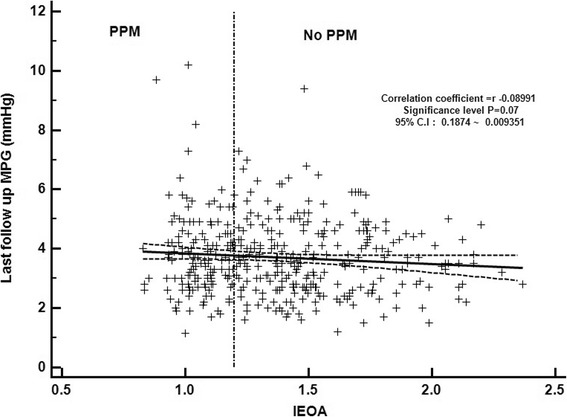
37% of patients (n = 165) had PPM. There were no significant differences in baseline and operative characteristics between patients with and without PPM except age and IEOA. A significant decrease in mean trans-valvular pressure gradient (MPG) over time following MVR, however the change of MPG showed no differences between groups (No PPM vs. PPM: 8.9 ± 4.7 mmHg → 3.6 ± 1.2 mmHg vs. 8.7 ± 4.5 mmHg → 3.8 ± 1.4 mmHg, p-value = 0.28). In all patients, there was a reduction of left atrium dimension (58.6 ± 12.0 mm → 53.2 ± 12.0 mm vs. 57.9 ± 8.9 mm → 52.2 ± 8.9 mm, p-value = 0.68) and left ventricular end diastolic diameter (49.9 ± 5.7 mm → 48.9 ± 5.7 mm vs. 49.7 ± 6.0 mm → 48.3 ± 5.0 mm, p = 0.24) without statistical significance. Freedom from TR progression rates at 3 and 5 years (99% vs.98%, 99% vs. 98%, p-value = 0.1), and overall survival rates at 3 and 5 years (97% vs. 96%, 94% vs. 94%, p-value = 0.7) were similar.
This study shows that mitral PPM is not associated with atrial /ventricular remodeling and might not influence late clinical outcome including late TR progression, survival in rheumatic population.
人工瓣膜-患者不匹配(PPM)的特征是相对于体表面积(BSA)而言人工瓣膜尺寸不足所产生的影响。本研究的目的是确定PPM对风湿性二尖瓣置换术(MVR)后晚期临床结局的影响。
对2000年至2013年期间共445例(平均年龄54.2±11.7岁)因风湿性疾病接受单纯MVR(±三尖瓣环成形术)的患者进行了调查。有效瓣口面积(EOA)通过连续方程确定,PPM定义为指数化EOA(EOA/BSA)≤1.2cm/m²。比较了临床和超声心动图随访(平均随访8.7±4.0年)结果。
37%的患者(n=165)存在PPM。有PPM和无PPM的患者在基线和手术特征方面无显著差异,但年龄和IEOA除外。MVR后平均跨瓣压差(MPG)随时间显著降低,然而两组间MPG的变化无差异(无PPM组与PPM组:8.9±4.7mmHg→3.6±1.2mmHg与8.7±4.5mmHg→3.8±1.4mmHg,p值=0.28)。在所有患者中,左心房内径(58.6±12.0mm→53.2±12.0mm与57.9±8.9mm→52.2±8.9mm,p值=0.68)和左心室舒张末期直径(49.9±5.7mm→48.9±5.7mm与49.7±6.0mm→48.3±5.0mm,p=0.24)均有减小,但无统计学意义。3年和5年无三尖瓣反流进展率(99%对98%,99%对98%,p值=0.1)以及3年和5年总生存率(97%对96%,94%对94%,p值=0.7)相似。
本研究表明,二尖瓣PPM与心房/心室重构无关,可能不影响包括晚期三尖瓣反流进展、风湿性患者生存率在内的晚期临床结局。