Goto Yasushi, Tanai Chiharu, Yoh Kiyotaka, Hosomi Yukio, Sakai Hiroshi, Kato Terufumi, Kaburagi Takayuki, Nishio Makoto, Kim Young Hak, Inoue Akira, Hasegawa Yoshinori, Isobe Hiroshi, Tomizawa Yoshio, Mori Yoshiaki, Minato Koichi, Yamada Kazuhiko, Ohashi Yasuo, Kunitoh Hideo
Department of Thoracic Oncology, National Cancer Center Hospital, Tokyo, Japan.
Division of Respirology, NTT Medical Center Tokyo, Tokyo, Japan.
ESMO Open. 2017 Sep 14;2(4):e000214. doi: 10.1136/esmoopen-2017-000214. eCollection 2017.
Some patients with advanced or recurrent, epidermal growth factor receptor (EGFR) mutation-positive (EGFR M+) non-small-cell lung cancer (NSCLC) continue to receive EGFR tyrosine kinase inhibitors (TKIs) beyond radiological progression.
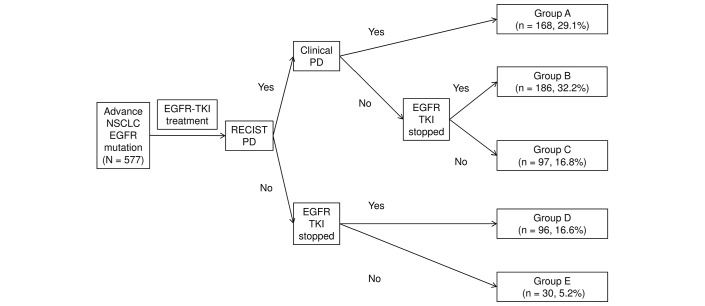
We analysed a cohort of 577 patients with EGFR M+ NSCLC, who had received a first-line EGFR-TKI. We classified patients according to clinical course and treatment patterns at Response Evaluation Criteria in Solid Tumors (RECIST) progressive disease (PD). We evaluated the period from RECIST PD to TKI discontinuation or clinical PD and also evaluated survival after RECIST PD and compared it between groups.
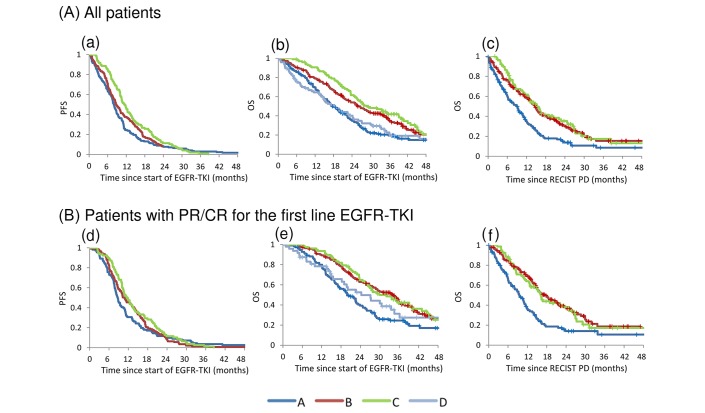
RECIST PD was documented in 451 cases, of which 283 (62.7%) were clinically stable. 186 (65.7%) discontinued and 97 (34.3%) continued the EGFR-TKI. In those who continued EGFR-TKI, median time between RECIST PD and clinical PD or TKI discontinuation was 5.1 months. Median survival after RECIST PD in patients who discontinued and continued EGFR-TKI after clinically stable RECIST PD was 14.6 and 15.3 months (p=0.5489), respectively. In multivariate analysis, continuing EGFR-TKI therapy, female gender, better performance status and exon 19 deletion subtype were likely positive predictive factors for survival after clinically stable RECIST PD.
Our study suggests that some patients could benefit from receiving an EGFR-TKI beyond radiological progression.
一些晚期或复发的表皮生长因子受体(EGFR)突变阳性(EGFR M+)非小细胞肺癌(NSCLC)患者在影像学进展后仍继续接受EGFR酪氨酸激酶抑制剂(TKIs)治疗。
我们分析了一组577例接受一线EGFR-TKI治疗的EGFR M+ NSCLC患者。我们根据实体瘤疗效评价标准(RECIST)中的疾病进展(PD)情况,对患者的临床病程和治疗模式进行分类。我们评估了从RECIST标准判定的PD到TKI停药或临床PD的时间,还评估了RECIST标准判定的PD后的生存期,并在组间进行比较。
451例患者记录有RECIST标准判定的PD,其中283例(62.7%)临床稳定。186例(65.7%)停用EGFR-TKI,97例(34.3%)继续使用EGFR-TKI。在继续使用EGFR-TKI的患者中,RECIST标准判定的PD至临床PD或TKI停药的中位时间为5.1个月。在RECIST标准判定的PD后,临床稳定的患者中,停用和继续使用EGFR-TKI的患者的中位生存期分别为14.6个月和15.3个月(p = 0.5489)。多因素分析显示,继续EGFR-TKI治疗、女性、较好的身体状况和外显子19缺失亚型可能是RECIST标准判定的临床稳定PD后生存的阳性预测因素。
我们的研究表明,一些患者在影像学进展后接受EGFR-TKI治疗可能会获益。