Yuan Kai-Ming, Fu Shu-Ying, Li Jun, Shangguan Wang-Ning, Lian Qing-Quan
Department of Anesthesiology and Perioperative Medicine, the Second Affiliated Hospital and Yuying Children's Hospital of Wenzhou Medical University, Wenzhou, China.
Medicine (Baltimore). 2017 Oct;96(41):e8304. doi: 10.1097/MD.0000000000008304.
Bezold-Jarisch reflex (BJR) occurs when the cardioinhibitory receptors in the walls of ventricles are activated by various stimuli, with typical features of bradycardia, vasorelaxation, and hypotension. This reflex usually happens in parturient intrathecal anesthesia, as a result of decreased venous return by compression of inferior vena cava, but it is only rarely reported during general anesthesia.
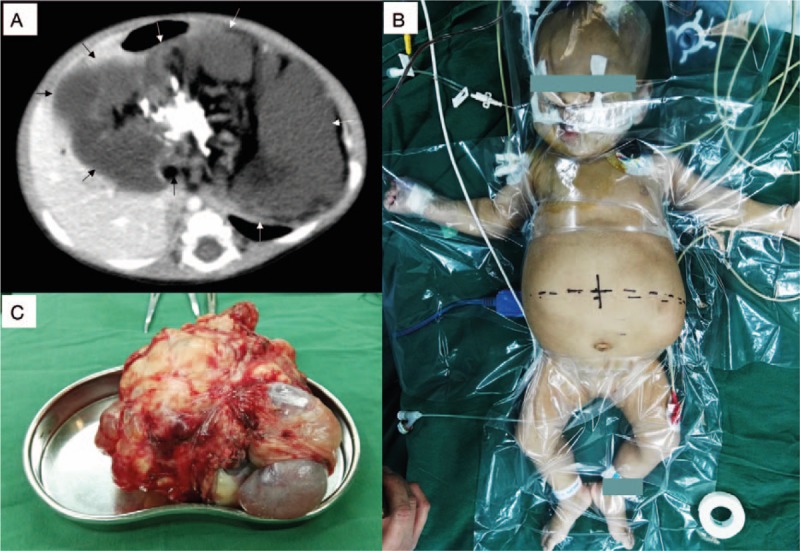
Severe bradycardia and hypotension, indicating BJR, occurred during the induction of general anesthesia in a 3-month-old female child with giant intra-abdominal teratoma.
A giant intra-abdominal teratoma was detected by computed tomography scanning. The decreased left ventricular ejection faction along with increased troponin I and N-terminal pro-B-type natriuretic peptide indicated a preoperative mild cardiac dysfunction. BJR was diagnosed on the basis of the severe bradycardia and hypotension observed during the induction of general anesthesia, INTERVENTIONS:: Atropine failed to increase heart rate. Cardiopulmonary resuscitation was initiated immediately and epinephrine was injected intravenously because of sudden circulatory collapse. Soon after the return of spontaneous circulation, a central venous line was placed and invasive blood pressure was monitored. Vital signs and homeostasis were kept stable during teratoma resection.
The child was extubated after emergence from anesthesia in the operating room. Eleven days later, she had recovered without complications and was discharged.
General anesthesia should be induced with great care in patients with giant intra-abdominal masses, and the patient should be kept in the left-lateral table tilt position before induction.
当心室壁中的心脏抑制感受器被各种刺激激活时,会发生贝佐尔德-雅里什反射(BJR),其典型特征为心动过缓、血管舒张和低血压。这种反射通常发生在产妇鞘内麻醉时,是下腔静脉受压导致静脉回流减少的结果,但在全身麻醉期间很少有报道。
一名患有巨大腹腔内畸胎瘤的3个月大女童在全身麻醉诱导期间出现严重心动过缓和低血压,提示发生了BJR。
通过计算机断层扫描检测到巨大腹腔内畸胎瘤。左心室射血分数降低以及肌钙蛋白I和N末端B型利钠肽原增加表明术前存在轻度心脏功能障碍。根据全身麻醉诱导期间观察到的严重心动过缓和低血压诊断为BJR。
阿托品未能提高心率。由于突然循环衰竭,立即开始心肺复苏并静脉注射肾上腺素。自主循环恢复后不久,放置中心静脉导管并监测有创血压。畸胎瘤切除期间生命体征和内环境保持稳定。
患儿在手术室麻醉苏醒后拔管。11天后,她康复且无并发症出院。
对于患有巨大腹腔内肿块的患者,应极其谨慎地诱导全身麻醉,诱导前患者应保持左侧卧位。