Department of Cardiology, Kanagawa Cardiovascular and Respiratory Center, Yokohama, Japan
Department of Cardiology, Keio University School of Medicine, Tokyo, Japan.
J Am Heart Assoc. 2017 Oct 11;6(10):e006431. doi: 10.1161/JAHA.117.006431.
Among patients treated with percutaneous coronary intervention for chronic total occlusion (CTO-PCI), patients on long-term hemodialysis are at significantly high risk for cardiovascular mortality and morbidity. However, clinical or angiographic predictors that might aid in better patient selection remain unclear. We aimed to assess the acute impact of hemodialysis in patients who underwent CTO-PCI.
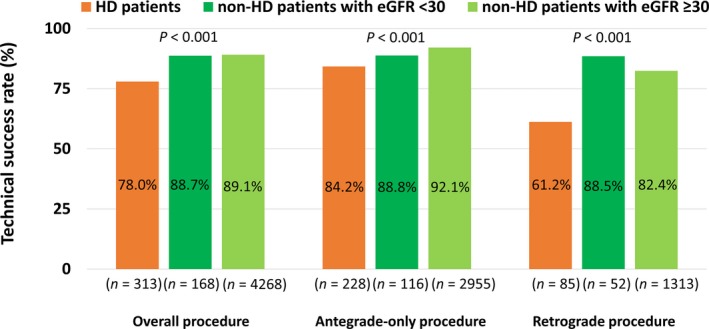
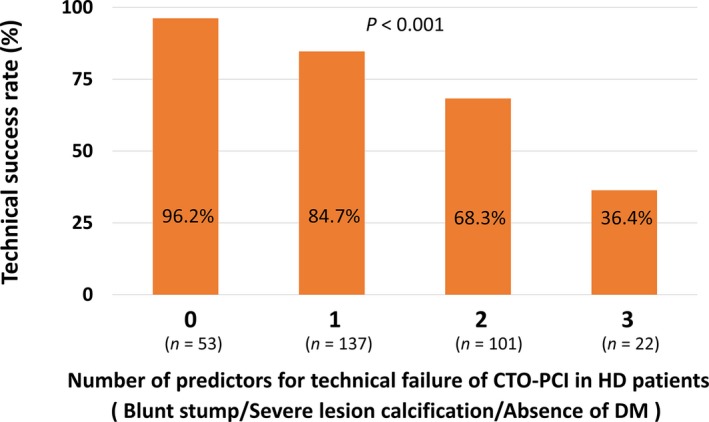
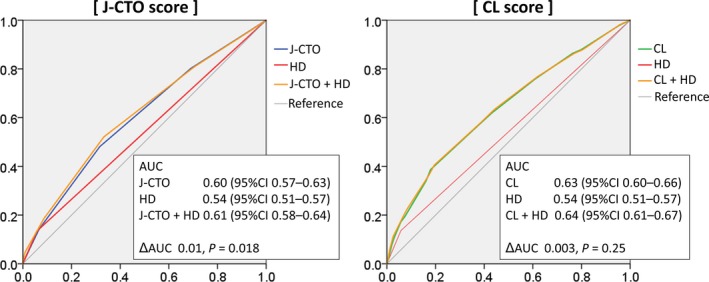
The Retrograde Summit registry is a multicenter, prospective registry of patients undergoing CTO-PCI at 65 Japanese centers. Patient characteristics and procedural outcomes of 4749 patients were analyzed, according to the presence (n=313) or absence (n=4436) of baseline hemodialysis. A prediction model for technical failure among hemodialysis patients was also developed. The technical success rate of CTO-PCI was significantly lower in hemodialysis than in nonhemodialysis patients (78.0% versus 89.1%, <0.001). The rates of in-hospital major adverse cardiac and cerebrovascular events were similar between the 2 groups (1.6% versus 0.9%, =0.24). Irrespective of clinical/angiographic characteristics or previously developed scoring systems, hemodialysis independently predicted technical failure for CTO-PCI. Among hemodialysis patients, predictors of technical failure were blunt stump (odds ratio 2.45, 95% confidence interval, 1.15-5.21, =0.021), severe lesion calcification (odds ratio 2.50, 95% confidence interval, 1.19-5.24, =0.015), and absence of diabetes mellitus (odds ratio 3.15, 95% confidence interval, 1.49-6.64, =0.003). In hemodialysis patients without these predictors, the technical success rate was 96.2%.
Hemodialysis is significantly associated with technical failure. Contemporary CTO-PCI seems feasible and safe in selected hemodialysis patients.
在接受慢性完全闭塞(CTO-PCI)经皮冠状动脉介入治疗的患者中,长期接受血液透析的患者心血管死亡率和发病率风险显著较高。然而,目前尚不清楚哪些临床或血管造影预测因素可能有助于更好地选择患者。我们旨在评估接受 CTO-PCI 的患者中血液透析的急性影响。
Retrograde Summit 注册研究是一项多中心、前瞻性研究,共纳入 65 家日本中心接受 CTO-PCI 的患者。根据基线时是否存在(n=313)或不存在(n=4436)血液透析,分析了 4749 例患者的患者特征和手术结果。还制定了血液透析患者技术失败的预测模型。与非血液透析患者相比,血液透析患者的 CTO-PCI 技术成功率明显较低(78.0%对 89.1%,<0.001)。两组住院期间主要不良心脏和脑血管事件的发生率相似(1.6%对 0.9%,=0.24)。无论临床/血管造影特征或之前开发的评分系统如何,血液透析均独立预测 CTO-PCI 的技术失败。在血液透析患者中,技术失败的预测因素为钝性残端(优势比 2.45,95%置信区间,1.15-5.21,=0.021)、严重病变钙化(优势比 2.50,95%置信区间,1.19-5.24,=0.015)和无糖尿病(优势比 3.15,95%置信区间,1.49-6.64,=0.003)。在没有这些预测因素的血液透析患者中,技术成功率为 96.2%。
血液透析与技术失败显著相关。在选定的血液透析患者中,现代 CTO-PCI 似乎是可行和安全的。