Cortez Daniel, Svensson Anneli, Carlson Jonas, Graw Sharon, Sharma Nandita, Brun Francesca, Spezzacatene Anita, Mestroni Luisa, Platonov Pyotr G
Department of Cardiology, Clinical Sciences, Lund University, Lund, Sweden.
Electrophysiology/Cardiology, Penn State Milton S. Hershey Medical Center, Hershey, USA.
BMC Cardiovasc Disord. 2017 Oct 13;17(1):261. doi: 10.1186/s12872-017-0696-x.
Arrhythmogenic right ventricular dysplasia/cardiomyopathy (ARVD/C) carries a risk of sudden death. We aimed to assess whether vectorcardiographic (VCG) parameters directed toward the right heart and a measured angle of the S-wave would help differentiate ARVD/C with otherwise normal electrocardiograms from controls.
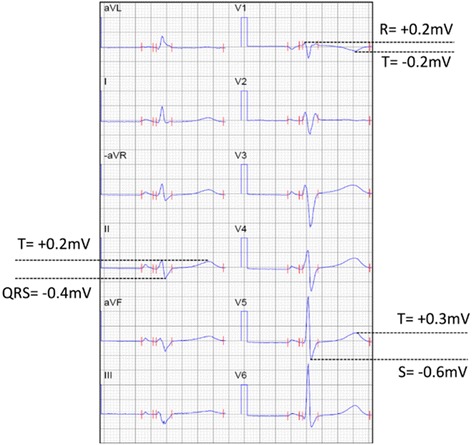
Task Force 2010 definite ARVD/C criteria were met for all patients. Those who did not fulfill Task Force depolarization or repolarization criteria (-ECG) were compared with age and gender-matched control subjects. Electrocardiogram measures of a 3-dimentional spatial QRS-T angle, a right-precordial-directed orthogonal QRS-T (RPD) angle, a root mean square of the right sided depolarizing forces (RtRMS-QRS), QRS duration (QRSd) and the corrected QT interval (QTc), and a measured angle including the upslope and downslope of the S-wave (S-wave angle) were assessed.
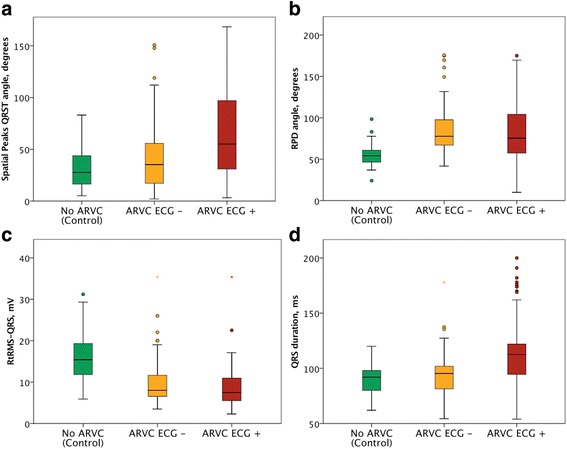
Definite ARVD/C was present in 155 patients by 2010 Task Force criteria (41.7 ± 17.6 years, 65.2% male). -ECG ARVD/C patients (66 patients) were compared to 66 control patients (41.7 ± 17.6 years, 65.2% male). All parameters tested except the QRSd and QTc significantly differentiated -ECG ARVD/C from control patients (p < 0.004 to p < 0.001). The RPD angle and RtRMS-QRS best differentiated the groups. Combined, the 2 novel criteria gave 81.8% sensitivity, 90.9% specificity and odds ratio of 45.0 (95% confidence interval 15.8 to 128.2).
ARVD/C disease process may lead to development of subtle ECG abnormalities that can be distinguishable using right-sided VCG or measured angle markers better than the spatial QRS-T angle, the QRSd or QTc, in the absence of Taskforce ECG criteria.
致心律失常性右室发育不良/心肌病(ARVD/C)存在猝死风险。我们旨在评估指向右心的向量心电图(VCG)参数及测量的S波角度是否有助于鉴别心电图正常的ARVD/C患者与对照组。
所有患者均符合2010年工作组确定的ARVD/C标准。将未满足工作组去极化或复极化标准(-ECG)的患者与年龄和性别匹配的对照受试者进行比较。评估三维空间QRS-T角度、右胸前导联定向正交QRS-T(RPD)角度、右侧去极化力均方根(RtRMS-QRS)、QRS波时限(QRSd)、校正QT间期(QTc)等心电图指标,以及包括S波上升支和下降支的测量角度(S波角度)。
根据2010年工作组标准,155例患者确诊为ARVD/C(41.7±17.6岁,65.2%为男性)。将-ECG ARVD/C患者(66例)与66例对照患者(41.7±17.6岁,65.2%为男性)进行比较。除QRSd和QTc外,所有测试参数均能显著区分-ECG ARVD/C患者与对照患者(p<0.004至p<0.001)。RPD角度和RtRMS-QRS对两组的区分效果最佳。综合这两个新指标,敏感性为81.8%,特异性为90.9%,优势比为45.0(95%置信区间15.8至128.2)。
在无工作组心电图标准的情况下,ARVD/C疾病过程可能导致细微的心电图异常,使用右侧VCG或测量角度标记比空间QRS-T角度、QRSd或QTc更能区分这些异常。