Yoon Jae-Ho, Kim Hee-Je, Kwak Dae-Hun, Min Gi June, Park Sung-Soo, Jeon Young-Woo, Lee Sung-Eun, Cho Byung-Sik, Eom Ki-Seong, Kim Yoo-Jin, Lee Seok, Min Chang-Ki, Cho Seok-Goo, Kim Dong-Wook, Lee Jong Wook, Min Woo-Sung
Department of Hematology, Catholic Blood and Marrow Transplantation Center, Leukemia Research Institute, Seoul St. Mary's Hospital, College of Medicine, The Catholic University of Korea, Seoul, Korea.
Blood Res. 2017 Sep;52(3):174-183. doi: 10.5045/br.2017.52.3.174. Epub 2017 Sep 25.
Standard remission induction chemotherapy consisting of anthracycline plus cytarabine (3+7) is administered for adult acute myeloid leukemia (AML). However, the effects of intensified regimen on complete remission (CR), relapse and overall survival (OS) remain unknown.
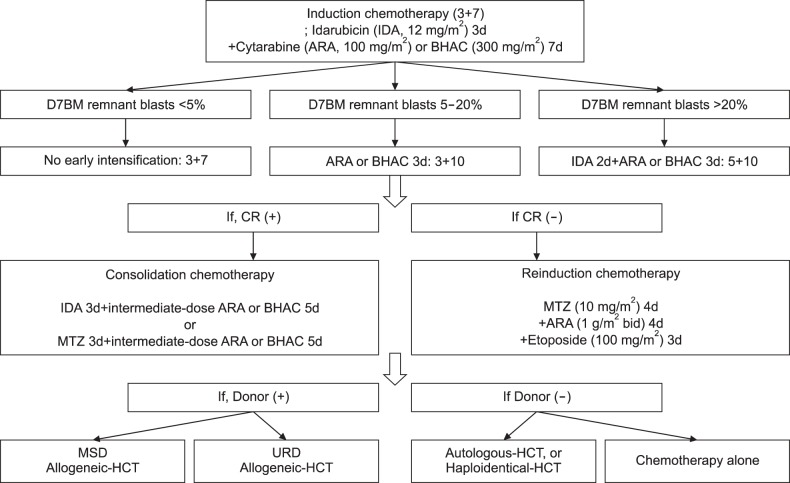
We analyzed 1195 patients treated with idarubicin plus cytarabine/BHAC (3+7) from 2002 to 2013. Among them, 731 received early intensification with 3-day cytarabine/BHAC (3+10, N=363) or 2-day idarubicin plus cytarabine/BHAC 3 days (5+10, N=368). The 3+10 and 5+10 strategies were applied to patients with bone marrow blast counts of 5-20% and >20% on day 7 of 3+7, respectively.
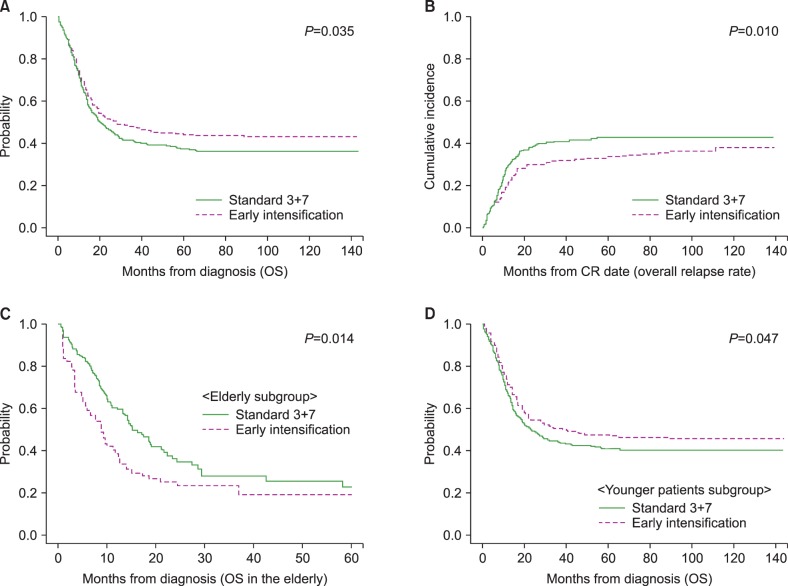
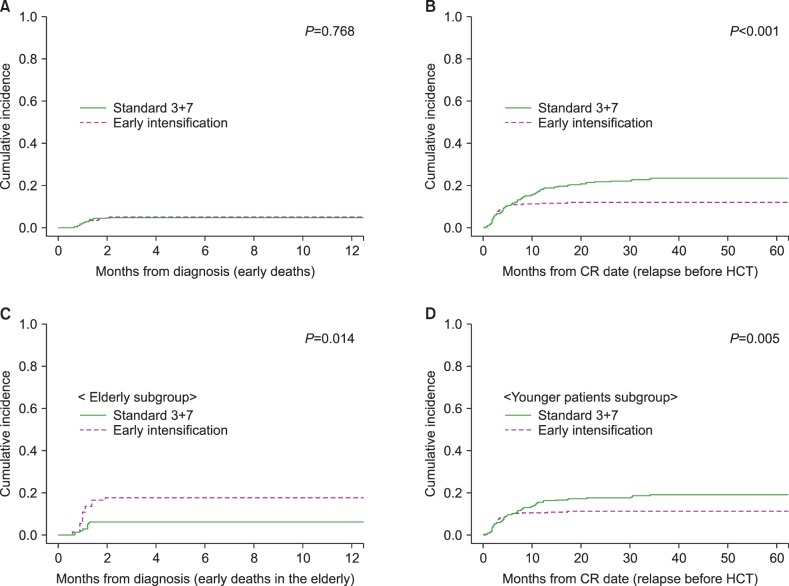
Early intensification correlated with a younger age (median: 40 vs. 45 yr) and higher t(8;21) frequency (20.4% vs. 7.1%), compared to 3+7. After early intensification, the early death rates were higher among the elderly (3+10 [15.7%], 5+10 [21.7%] vs. 3+7 [6.3%], =0.038), while the post-induction CR rate was higher in young patients (3+10 [79.8%], 5+10 [75.1%] vs. 3+7 [65.1%], <0.001). Early relapse rate was also decreased (3+10 [11.8%], 5+10 [11.7%] vs. 3+7 [22.0%], <0.001). In multivariate analysis, early intensification correlated with an inferior 5-year OS among elderly patients (19.2% vs. 22.8%; hazard ratio [HR]=1.84, 95% confidence interval [CI]; 1.11-3.06, =0.018) and lower overall relapse rate among young patients (33.0% vs. 41.4%, =0.023; HR=0.71, 95% CI; 0.55-0.93, =0.012).
Early intensification correlated with higher CR and lower relapse rates, but not OS in young AML patients. In elderly patients, early intensification correlated with a higher early death rate and poorer OS.
成人急性髓系白血病(AML)的标准缓解诱导化疗方案为蒽环类药物联合阿糖胞苷(3+7)。然而,强化方案对完全缓解(CR)、复发及总生存期(OS)的影响尚不清楚。
我们分析了2002年至2013年期间接受伊达比星联合阿糖胞苷/BHAC(3+7)治疗的1195例患者。其中,731例接受了早期强化治疗,采用3天阿糖胞苷/BHAC(3+10,n=363)或3天2天伊达比星联合阿糖胞苷/BHAC(5+10,n=368)。3+10和5+10策略分别应用于3+7方案第7天骨髓原始细胞计数为5%-20%和>20%的患者。
与3+7方案相比,早期强化治疗的患者年龄较轻(中位年龄:40岁对45岁),t(8;21)频率较高(20.4%对7.1%)。早期强化治疗后,老年患者的早期死亡率较高(3+10[15.7%],5+10[21.7%]对3+7[6.3%],P=0.038),而年轻患者诱导后CR率较高(3+10[79.8%],5+10[75.1%]对3+7[65.1%],P<0.001)。早期复发率也有所降低(3+10[11.8%],5+10[11.7%]对3+7[22.0%],P<0.001)。多因素分析显示,早期强化治疗与老年患者较差的5年总生存期相关(19.2%对22.8%;风险比[HR]=1.84,95%置信区间[CI]:1.11-3.06,P=0.018),与年轻患者较低的总体复发率相关(33.0%对41.4%,P=0.023;HR=0.71,95%CI:0.55-0.93,P=0.012)。
早期强化治疗与年轻AML患者较高的CR率和较低的复发率相关,但与总生存期无关。在老年患者中,早期强化治疗与较高的早期死亡率和较差的总生存期相关。