Baksaas-Aasen Kjersti, Gall Lewis, Eaglestone Simon, Rourke Claire, Juffermans Nicole P, Goslings J Carel, Naess Paal Aksel, van Dieren Susan, Ostrowski Sisse Rye, Stensballe Jakob, Maegele Marc, Stanworth Simon J, Gaarder Christine, Brohi Karim, Johansson Per I
Department of Traumatology, Oslo University Hospital, Oslo, Norway.
Centre for Trauma Sciences, Blizard Institute, Queen Mary University of London, London, UK.
Trials. 2017 Oct 18;18(1):486. doi: 10.1186/s13063-017-2224-9.
Traumatic injury is the fourth leading cause of death globally. Half of all trauma deaths are due to bleeding and most of these will occur within 6 h of injury. Haemorrhagic shock following injury has been shown to induce a clotting dysfunction within minutes, and this early trauma-induced coagulopathy (TIC) may exacerbate bleeding and is associated with higher mortality and morbidity. In spite of improved resuscitation strategies over the last decade, current transfusion therapy still fails to correct TIC during ongoing haemorrhage and evidence for the optimal management of bleeding trauma patients is lacking. Recent publications describe increasing the use of Viscoelastic Haemostatic Assays (VHAs) in trauma haemorrhage; however, there is insufficient evidence to support their superiority to conventional coagulation tests (CCTs).
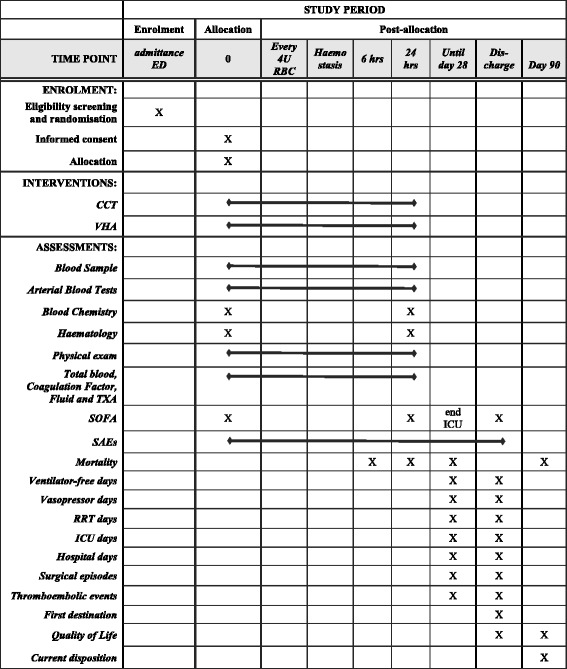
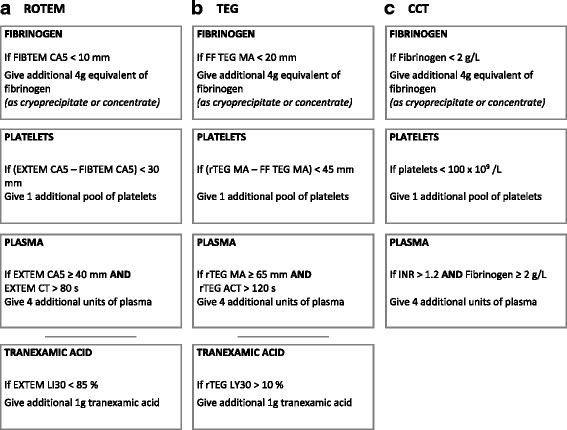
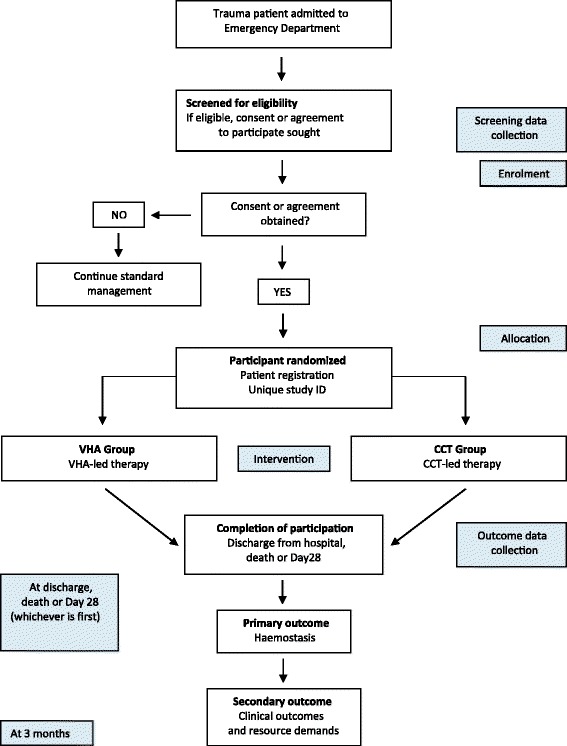
METHODS/DESIGN: This multicentre, randomised controlled study will compare the haemostatic effect of an evidence-based VHA-guided versus an optimised CCT-guided transfusion algorithm in haemorrhaging trauma patients. A total of 392 adult trauma patients will be enrolled at major trauma centres. Participants will be eligible if they present with clinical signs of haemorrhagic shock, activate the local massive haemorrhage protocol and initiate first blood transfusion. Enrolled patients will be block randomised per centre to either VHA-guided or CCT-guided transfusion therapy in addition to that therapy delivered as part of standard care, until haemostasis is achieved. Patients will be followed until discharge or 28 days. The primary endpoint is the proportion of subjects alive and free of massive transfusion (less than 10 units of red blood cells) at 24 h. Secondary outcomes include the effect of CCT- versus VHA-guided therapy on organ failure, total hospital and intensive care lengths of stay, health care resources needed and mortality. Surviving patients will be asked to complete a quality of life questionnaire (EuroQol EQ-5D) at day 90.
CCTs have traditionally been used to detect TIC and monitor response to treatment in traumatic major haemorrhage. The use of VHAs is increasing, but limited evidence exists to support the superiority of these technologies (or comparatively) for patient-centred outcomes. This knowledge gap will be addressed by this trial.
ClinicalTrials.gov, ID: NCT02593877 . Registered on 15 October 2015. Trial sponsor Queen Mary University of London The contact person of the above sponsor organisation is: Dr. Sally Burtles, Director of Research Services and Business Development, Joint Research Management Office, QM Innovation Building, 5 Walden Street, London E1 2EF; phone: 020 7882 7260; Email: sponsorsrep@bartshealth.nhs.uk Trial sites Academic Medical Centre, Amsterdam, The Netherlands Kliniken der Stadt Köln gGmbH, Cologne, Germany Rigshospitalet (Copenhagen University Hospital), Copenhagen, Denmark John Radcliff Hospital, Oxford, United Kingdom Oslo University Hospital, Oslo, Norway The Royal London Hospital, London, United Kingdom Centre for Trauma Sciences, Blizard Institute, Queen Mary University of London, London, United Kingdom Health Economics Research Centre, Nuffield Department of Population Health, University of Oxford, Oxford, United Kingdom Sites that are planning to start recruitment in mid/late 2017 Nottingham University Hospitals, Queen's Medical Centre, Nottingham, United Kingdom University of Kansas Hospital (UKH), Kansas City, MO, USA Protocol version: 3.0/14.03.2017 (Additional file 1).
创伤性损伤是全球第四大死因。所有创伤死亡病例中有一半是由于出血,其中大多数将在受伤后6小时内发生。受伤后的失血性休克已被证明在几分钟内就会引发凝血功能障碍,这种早期创伤性凝血病(TIC)可能会加剧出血,并与更高的死亡率和发病率相关。尽管在过去十年中复苏策略有所改进,但目前的输血治疗在持续出血期间仍无法纠正TIC,并且缺乏针对出血性创伤患者最佳管理的证据。最近的出版物描述了在创伤性出血中增加使用粘弹性止血检测(VHA);然而,没有足够的证据支持其优于传统凝血试验(CCT)。
方法/设计:这项多中心随机对照研究将比较基于证据的VHA指导与优化的CCT指导的输血算法在出血性创伤患者中的止血效果。共有392名成年创伤患者将在主要创伤中心入组。如果参与者出现失血性休克的临床体征、启动当地大规模出血方案并开始首次输血,则符合入选条件。入组患者将在每个中心进行区组随机分组,接受VHA指导或CCT指导的输血治疗,此外还将接受作为标准治疗一部分提供的治疗,直至实现止血。患者将被随访至出院或28天。主要终点是24小时时存活且未接受大量输血(少于10单位红细胞)的受试者比例。次要结局包括CCT指导与VHA指导治疗对器官衰竭、总住院时间和重症监护住院时间、所需医疗资源和死亡率的影响。存活患者将被要求在第90天完成一份生活质量问卷(欧洲五维度健康量表EQ-5D)。
传统上,CCT一直用于检测TIC并监测创伤性大出血的治疗反应。VHA的使用正在增加,但支持这些技术(或相对而言)在以患者为中心的结局方面具有优越性的证据有限。本试验将填补这一知识空白。
ClinicalTrials.gov,标识符:NCT02593877。于2015年10月15日注册。试验主办方:伦敦玛丽女王大学 上述主办方组织的联系人是:研究服务与业务发展主任Sally Burtles博士,联合研究管理办公室,QM创新大楼,伦敦沃尔登街5号,E1 2EF;电话:020 7882 7260;电子邮件:sponsorsrep@bartshealth.nhs.uk 试验地点 荷兰阿姆斯特丹学术医疗中心 德国科隆市立医院有限公司,科隆,德国 丹麦哥本哈根大学医院里格医院 英国牛津约翰·拉德克利夫医院 挪威奥斯陆大学医院,奥斯陆 英国伦敦皇家伦敦医院 英国伦敦玛丽女王大学布莱兹研究所创伤科学中心 英国牛津大学纳菲尔德人口健康系卫生经济研究中心 计划于2017年年中/年末开始招募的地点 英国诺丁汉大学医院女王医疗中心,诺丁汉 美国密苏里州堪萨斯城堪萨斯大学医院(UKH) 方案版本:3.0/2017年3月14日(补充文件1)