Department of Medical Sciences, Cardiology, Uppsala University, Uppsala, Sweden.
Uppsala Clinical Research Center, Uppsala University, Uppsala, Sweden.
Eur Heart J. 2018 Feb 7;39(6):477-485. doi: 10.1093/eurheartj/ehx584.
In atrial fibrillation (AF), mortality remains high despite effective anticoagulation. A model predicting the risk of death in these patients is currently not available. We developed and validated a risk score for death in anticoagulated patients with AF including both clinical information and biomarkers.
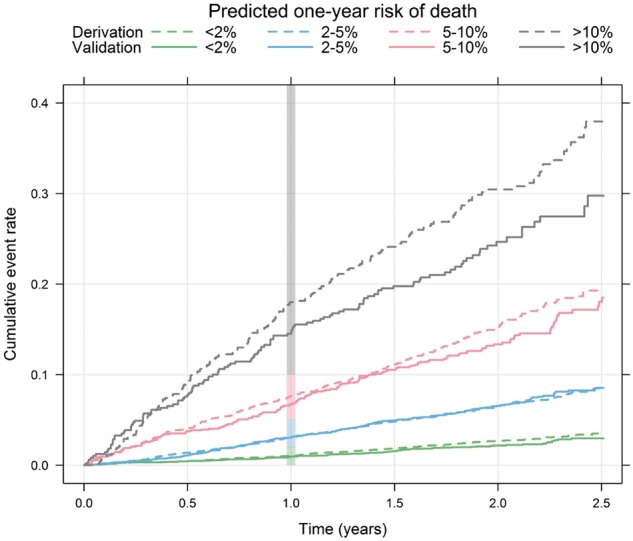
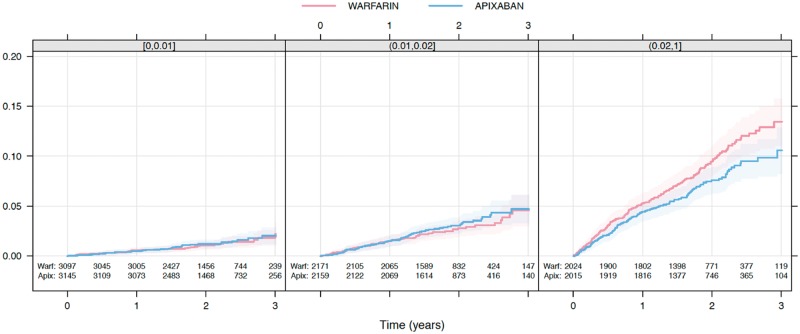
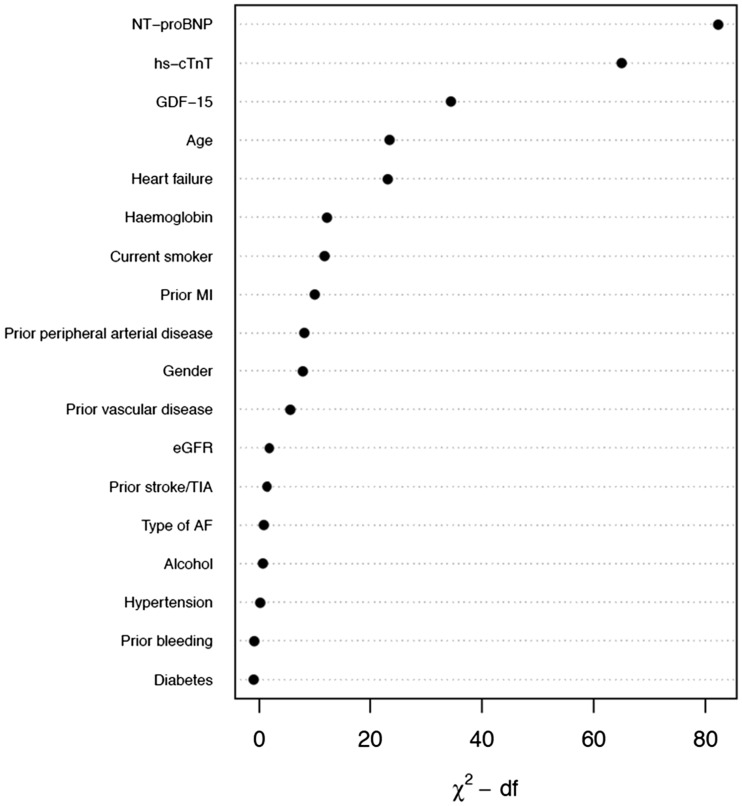
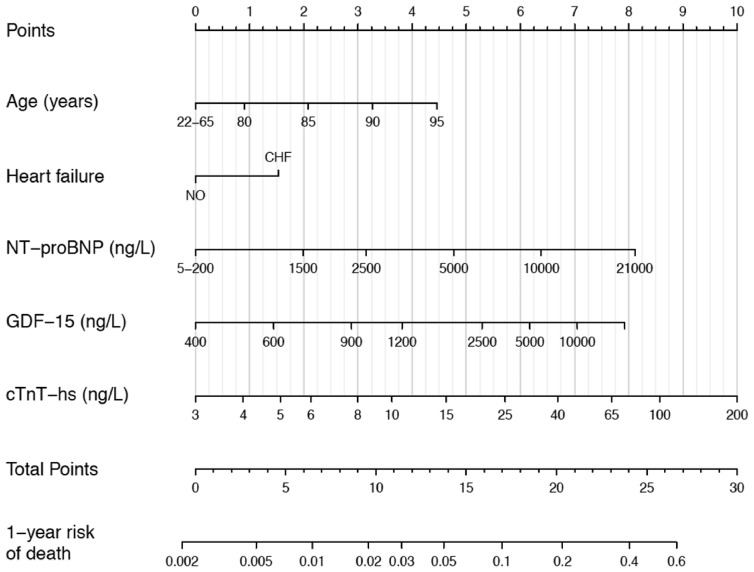
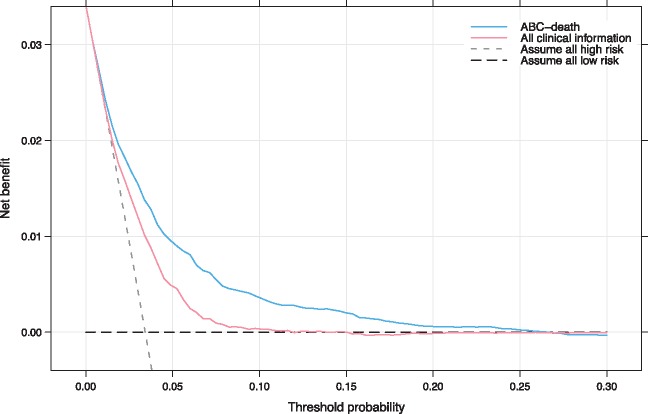
The new risk score was developed and internally validated in 14 611 patients with AF randomized to apixaban vs. warfarin for a median of 1.9 years. External validation was performed in 8548 patients with AF randomized to dabigatran vs. warfarin for 2.0 years. Biomarker samples were obtained at study entry. Variables significantly contributing to the prediction of all-cause mortality were assessed by Cox-regression. Each variable obtained a weight proportional to the model coefficients. There were 1047 all-cause deaths in the derivation and 594 in the validation cohort. The most important predictors of death were N-terminal pro B-type natriuretic peptide, troponin-T, growth differentiation factor-15, age, and heart failure, and these were included in the ABC (Age, Biomarkers, Clinical history)-death risk score. The score was well-calibrated and yielded higher c-indices than a model based on all clinical variables in both the derivation (0.74 vs. 0.68) and validation cohorts (0.74 vs. 0.67). The reduction in mortality with apixaban was most pronounced in patients with a high ABC-death score.
A new biomarker-based score for predicting risk of death in anticoagulated AF patients was developed, internally and externally validated, and well-calibrated in two large cohorts. The ABC-death risk score performed well and may contribute to overall risk assessment in AF.
CLINICALTRIALS.GOV IDENTIFIER: NCT00412984 and NCT00262600.
尽管进行了有效的抗凝治疗,心房颤动(AF)患者的死亡率仍然很高。目前尚无预测此类患者死亡风险的模型。我们开发并验证了一种用于预测接受抗凝治疗的 AF 患者死亡风险的风险评分,该评分包含临床信息和生物标志物。
新的风险评分在 14611 例接受阿哌沙班或华法林治疗的 AF 患者中进行了开发和内部验证,中位随访时间为 1.9 年。在 8548 例接受达比加群或华法林治疗 2.0 年的 AF 患者中进行了外部验证。在研究入组时获得了生物标志物样本。通过 Cox 回归评估对全因死亡率有显著预测作用的变量。每个变量都根据模型系数获得一个权重。在推导队列中有 1047 例全因死亡,验证队列中有 594 例全因死亡。死亡的最重要预测因素是 N 端脑利钠肽前体、肌钙蛋白 T、生长分化因子 15、年龄和心力衰竭,这些因素包含在 ABC(年龄、生物标志物、临床病史)-死亡风险评分中。评分具有良好的校准度,并且在推导队列(0.74 比 0.68)和验证队列(0.74 比 0.67)中均比基于所有临床变量的模型得出的 C 指数更高。在高 ABC-死亡评分的患者中,阿哌沙班降低死亡率的效果最为明显。
我们开发了一种新的基于生物标志物的评分,用于预测接受抗凝治疗的 AF 患者的死亡风险,该评分在两个大型队列中进行了内部和外部验证,并且具有良好的校准度。ABC-死亡风险评分表现良好,可能有助于 AF 的总体风险评估。
NCT00412984 和 NCT00262600。