Xu Jianping, Liu Xiaoyan, Yang Sheng, Zhang Xiangru, Shi Yuankai
Department of Medical Oncology, National Cancer Center/Cancer Hospital, Chinese Academy of Medical Sciences & Peking Union Medical College, Beijing Key Laboratory of Clinical Study on Anticancer Molecular Targeted Drugs, Beijing, People's Republic of China.
Onco Targets Ther. 2017 Oct 13;10:4989-4995. doi: 10.2147/OTT.S142686. eCollection 2017.
Treatment failure frequently occurs in patients with epidermal growth factor receptor (EGFR)-mutant non-small cell lung cancer (NSCLC) who respond to EGFR tyrosine kinase inhibitors initially. This retrospective study tried to investigate the efficacy and safety of apatinib plus icotinib in patients with advanced NSCLC after icotinib treatment failure.
This study comprised 27 patients with advanced NSCLC who had progressed after icotinib monotherapy. Initially, patients received oral icotinib (125 mg, tid) alone. When the disease progressed, they received icotinib plus apatinib (500 mg, qd, orally). Treatment was continued until disease progression, unacceptable toxicity or consent withdrawal.
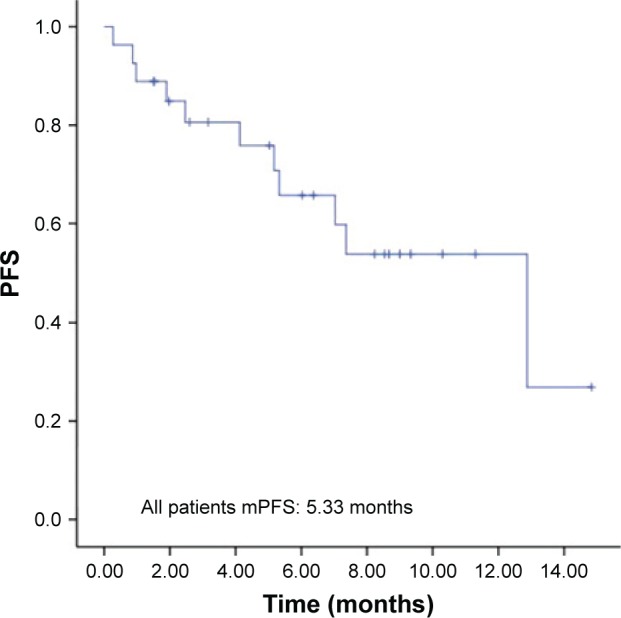
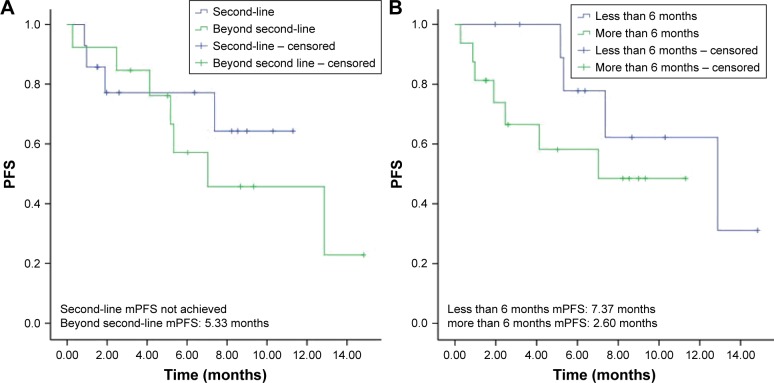
Followed up to December 2016, the median time of combined therapy was 7.47 months, and eight of 27 patients were dead. The median overall survival was not reached, and median progression-free survival (PFS) was 5.33 months (95% CI, 3.63-7.03 months). Moreover, the objective response rate (ORR) was 11.1%, and the disease control rate (DCR) was 81.5%. A total of 14 patients received combined therapy as the second-line treatment, and the ORR and DCR were 7.1% and 78.6%, respectively; 13 patients received drugs as the third- or later-line treatment, with an ORR and a DCR of 15.4% and 84.6%, respectively. In addition, 11 patients experienced icotinib monotherapy failure within 6 months with median PFS of 7.37 months, and 16 patients had progression after 6 months with median PFS of 2.60 months. The common drug-related toxic effects were hypertension (44.4%) and fatigue (37.0%).
Apatinib plus icotinib is efficacious in treating patients with advanced NSCLC after icotinib treatment failure, with acceptable toxic effects.
表皮生长因子受体(EGFR)突变的非小细胞肺癌(NSCLC)患者在最初对EGFR酪氨酸激酶抑制剂有反应后,治疗失败经常发生。这项回顾性研究试图探讨阿帕替尼联合埃克替尼治疗埃克替尼治疗失败后的晚期NSCLC患者的疗效和安全性。
本研究纳入27例埃克替尼单药治疗后病情进展的晚期NSCLC患者。最初,患者仅接受口服埃克替尼(125mg,每日三次)。当疾病进展时,他们接受埃克替尼联合阿帕替尼(500mg,每日一次,口服)。治疗持续至疾病进展、出现不可接受的毒性或患者撤回同意。
随访至2016年12月,联合治疗的中位时间为7.47个月,27例患者中有8例死亡。中位总生存期未达到,中位无进展生存期(PFS)为5.33个月(95%CI,3.63 - 7.03个月)。此外,客观缓解率(ORR)为11.1%,疾病控制率(DCR)为81.5%。共有14例患者接受联合治疗作为二线治疗,ORR和DCR分别为7.1%和78.6%;13例患者接受联合治疗作为三线或更后线治疗,ORR和DCR分别为15.4%和84.6%。此外,11例患者在6个月内出现埃克替尼单药治疗失败,中位PFS为7.37个月,16例患者在6个月后出现病情进展,中位PFS为2.60个月。常见的药物相关毒性反应为高血压(44.4%)和疲劳(37.0%)。
阿帕替尼联合埃克替尼治疗埃克替尼治疗失败后的晚期NSCLC患者有效,且毒性反应可接受。