Department of Urology, Medical University of Vienna, Vienna, Austria.
Division of General and Pediatric Radiology, Department of Biomedical Imaging and Image-guided Therapy, Medical University of Vienna, Vienna, Austria.
Eur J Nucl Med Mol Imaging. 2018 Feb;45(2):235-242. doi: 10.1007/s00259-017-3858-2. Epub 2017 Oct 26.
To evaluate the diagnostic performance of [Ga]Ga-PSMA conjugate 11 positron emission tomography (PSMA-PET) in the early detection of metastases in patients with biochemical recurrence (BCR) after radical prostatectomy (RP) for clinically non-metastatic prostate cancer, to compare it to CT/MRI alone and to assess its impact on further therapeutic decisions.
We retrospectively assessed 117 consecutive hormone-naïve BCR patients who had Ga-PSMA 11 PET/CT (n = 46) or PET/MRI (n = 71) between May 2014 and January 2017. BCR was defined as two PSA rises above 0.2 ng/ml. Two dedicated uro-oncological imaging experts (radiology/nuclear medicine) reviewed separately all images. All results were presented in a blinded sequential fashion to a multidisciplinary tumorboard in order to assess the influence of PSMA-PET imaging on decision-making.
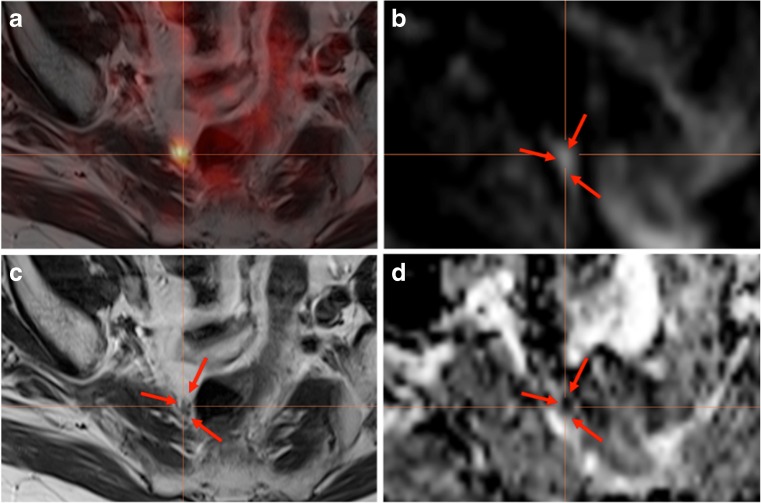
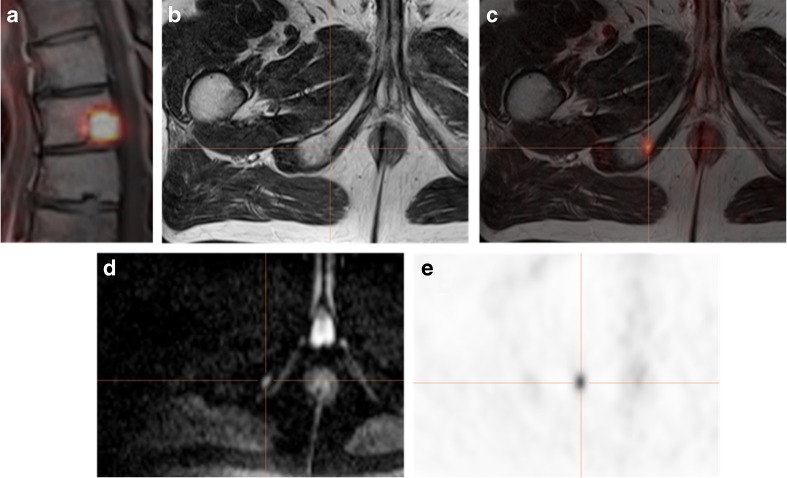
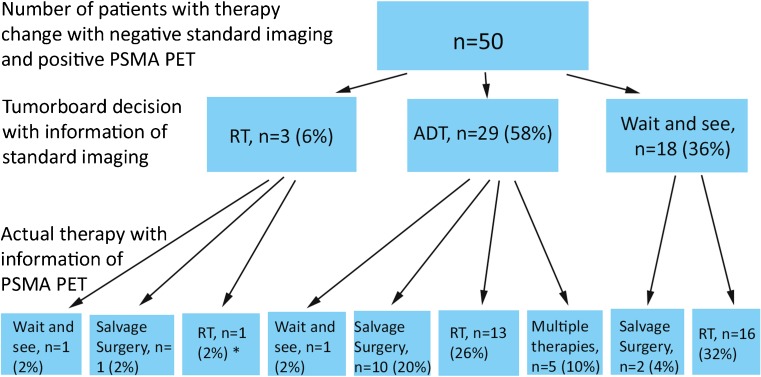
The median time from RP to BCR was 36 months (IQR 16-72). Overall, 69 (59%) patients received postoperative radiotherapy. Median PSA level at the time of imaging was 1.04 ng/ml (IQR 0.58-1.87). PSMA-positive lesions were detected in 100 (85.5%) patients. Detection rates were 65% for a PSA value of 0.2 to <0.5 ng/ml, 85.7% for 0.5 to <1, 85.7% for 1 to <2 and 100% for ≥2. PSMA-positive lesions could be confirmed by either histology (16%), PSA decrease in metastasis-directed radiotherapy (45%) or additional information in diffusion-weighted imaging when PET/MRI was performed (18%) in 79% of patients. PSMA-PET detected lesions in 67 patients (57.3%) who had no suspicious correlates according to the RECIST 1.1 criteria on MRI or CT. PSMA-PET changed therapeutic decisions in 74.6% of these 67 patients (p < 0.001), with 86% of them being considered for metastases-directed therapies.
We confirm the high performance of PSMA-PET imaging for the detection of disease recurrence sites in patients with BCR after RP, even at relatively low PSA levels. Moreover, it adds significant information to standard CT/MRI, changing treatment strategies in a significant number of patients.
评估 [Ga]Ga-PSMA 缀合物 11 正电子发射断层扫描(PSMA-PET)在经根治性前列腺切除术(RP)治疗后临床无转移前列腺癌生化复发(BCR)患者中转移的早期检测中的诊断性能,将其与 CT/MRI 单独检查进行比较,并评估其对进一步治疗决策的影响。
我们回顾性评估了 2014 年 5 月至 2017 年 1 月期间进行 Ga-PSMA 11 PET/CT(n=46)或 PET/MRI(n=71)的 117 例连续的激素初治 BCR 患者。BCR 定义为 PSA 两次升高超过 0.2ng/ml。两位专门的泌尿肿瘤影像学专家(放射科/核医学科)分别单独对所有图像进行了评估。所有结果均以盲法顺序呈现给多学科肿瘤委员会,以评估 PSMA-PET 成像对决策的影响。
从 RP 到 BCR 的中位时间为 36 个月(IQR 16-72)。总体而言,69 例(59%)患者接受了术后放疗。影像学检查时的中位 PSA 水平为 1.04ng/ml(IQR 0.58-1.87)。100 例(85.5%)患者的 PSMA 阳性病变。PSA 值为 0.2 至 <0.5ng/ml 时的检出率为 65%,0.5 至 <1ng/ml 时为 85.7%,1 至 <2ng/ml 时为 85.7%,≥2ng/ml 时为 100%。PSMA 阳性病变可通过组织学(16%)、转移定向放疗中 PSA 下降(45%)或当进行 PET/MRI 时扩散加权成像中的附加信息(18%)在 79%的患者中得到确认。PSMA-PET 在 67 例(57.3%)患者中检测到病变,这些患者在 MRI 或 CT 上根据 RECIST 1.1 标准无可疑相关性。PSMA-PET 改变了这些 67 例患者中的 74.6%(p<0.001)的治疗决策,其中 86%的患者被考虑进行转移定向治疗。
我们证实 PSMA-PET 成像在检测 RP 后 BCR 患者疾病复发部位方面具有较高的性能,即使在相对较低的 PSA 水平下也是如此。此外,它为标准 CT/MRI 添加了重要信息,改变了大量患者的治疗策略。