Department of Epidemiology and Biostatistics, School of Public Health, Imperial College London, St. Mary's Campus, Norfolk Place, Paddington, London, W2 1PG, UK.
Biostatistics Unit, Centre for Epidemiology and Biostatistics, University of Leeds, Leeds, UK.
Eur J Nutr. 2018 Aug;57(5):1701-1720. doi: 10.1007/s00394-017-1557-1. Epub 2017 Oct 28.
There is no published dose-response meta-analysis on the association between height and colorectal cancer risk (CRC) by sex and anatomical sub-site. We conducted a meta-analysis of prospective studies on the association between height and CRC risk with subgroup analysis and updated evidence on the association between body fatness and CRC risk.
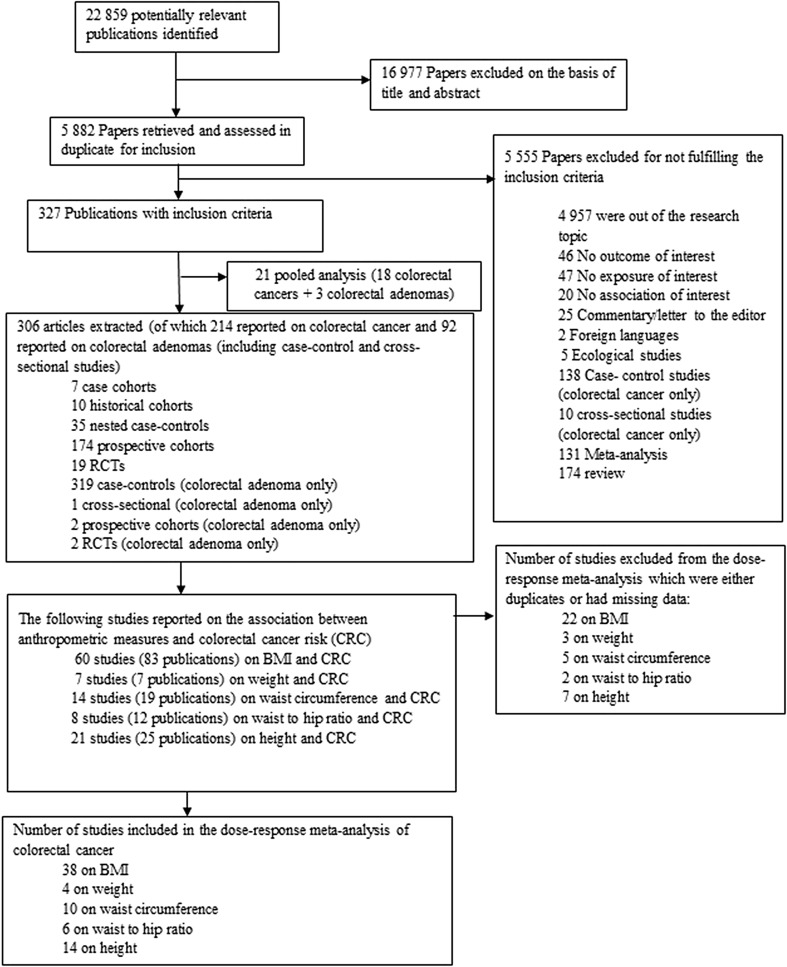
PubMed and several other databases were searched up to November 2016. A random effects model was used to calculate dose-response summary relative risks (RR's).
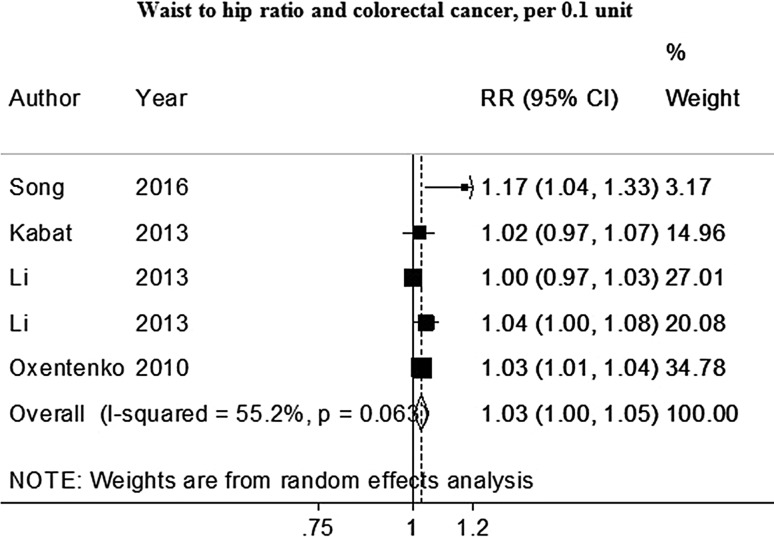
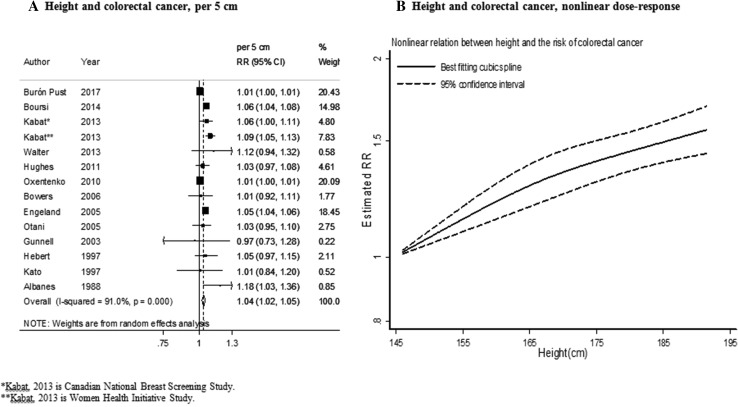
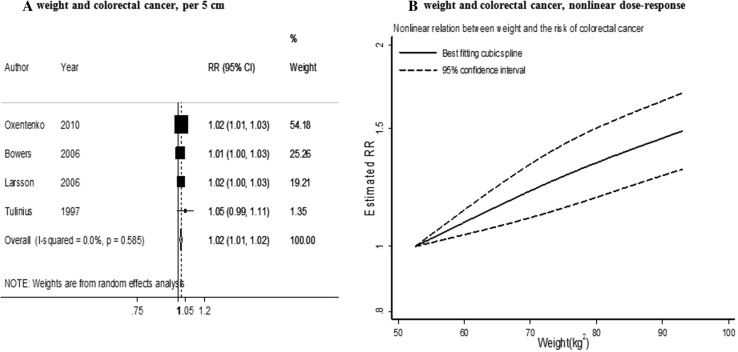
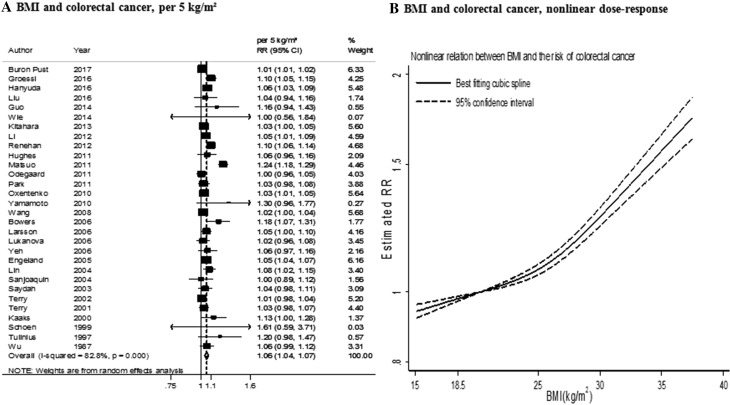
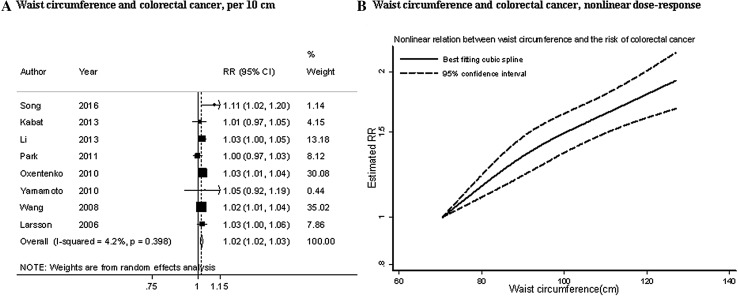
47 studies were included in the meta-analyses including 50,936 cases among 7,393,510 participants. The findings support the existing evidence regarding a positive association of height, general and abdominal body fatness and CRC risk. The summary RR were 1.04 [95% (CI)1.02-1.05, I² = 91%] per 5 cm increase in height, 1.02 [95% (CI)1.01-1.02, I² = 0%] per 5 kg increase in weight, 1.06 [95% (CI)1.04-1.07, I² = 83%] per 5 kg/m increase in BMI, 1.02 [95% (CI)1.02-1.03, I² = 4%] per 10 cm increase in waist circumference, 1.03 [95% (CI)1.01-1.05, I² = 16%] per 0.1 unit increase in waist to hip ratio. The significant association for height and CRC risk was similar in men and women. The significant association for BMI and CRC risk was stronger in men than in women.
The positive association between height and risk of CRC suggests that life factors during childhood and early adulthood might play a role in CRC aetiology. Higher general and abdominal body fatness during adulthood are risk factors of CRC and these associations are stronger in men than in women.
目前尚无关于身高与结直肠癌风险(CRC)性别和解剖亚部位关系的已发表剂量-反应荟萃分析。我们对前瞻性研究进行了荟萃分析,以评估身高与 CRC 风险之间的关系,并进行了亚组分析和更新的身体肥胖与 CRC 风险之间关系的证据。
检索了 PubMed 和其他几个数据库,截至 2016 年 11 月。使用随机效应模型计算剂量-反应汇总相对风险(RR)。
共有 47 项研究纳入荟萃分析,包括 7393510 名参与者中的 50936 例病例。研究结果支持了现有证据,即身高、全身和腹部体脂与 CRC 风险呈正相关。身高每增加 5cm,RR 为 1.04[95%(CI)1.02-1.05,I²=91%];体重每增加 5kg,RR 为 1.02[95%(CI)1.01-1.02,I²=0%];BMI 每增加 5kg/m,RR 为 1.06[95%(CI)1.04-1.07,I²=83%];腰围每增加 10cm,RR 为 1.02[95%(CI)1.02-1.03,I²=4%];腰围臀围比每增加 0.1 单位,RR 为 1.03[95%(CI)1.01-1.05,I²=16%]。身高与 CRC 风险之间的显著相关性在男性和女性中相似。BMI 与 CRC 风险之间的显著相关性在男性中强于女性。
身高与 CRC 风险之间的正相关表明,儿童期和成年早期的生活因素可能在 CRC 的发病机制中起作用。成年期更高的全身和腹部体脂是 CRC 的危险因素,这些关联在男性中强于女性。