Department of Health Technology and Informatics, The Hong Kong Polytechnic University, Hung Hom, Kowloon, Hong Kong, SAR, China.
Department of Surgery, Prince of Wales Hospital, The Chinese University of Hong Kong, Shatin, New Territories, Hong Kong, SAR, China.
Sci Rep. 2017 Oct 30;7(1):14350. doi: 10.1038/s41598-017-14432-7.
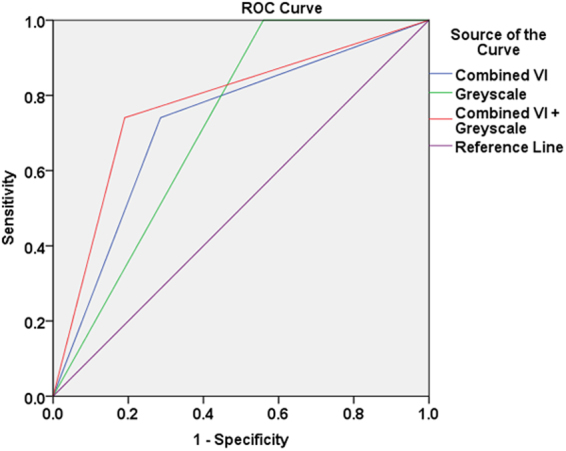
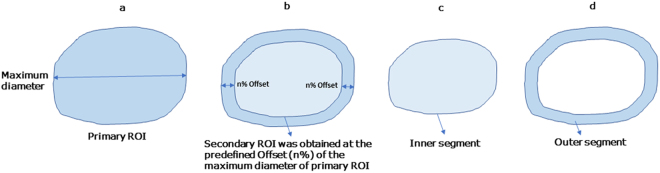
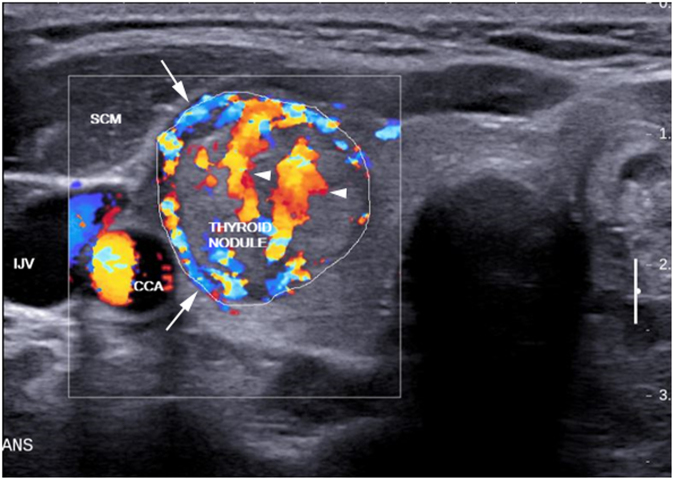
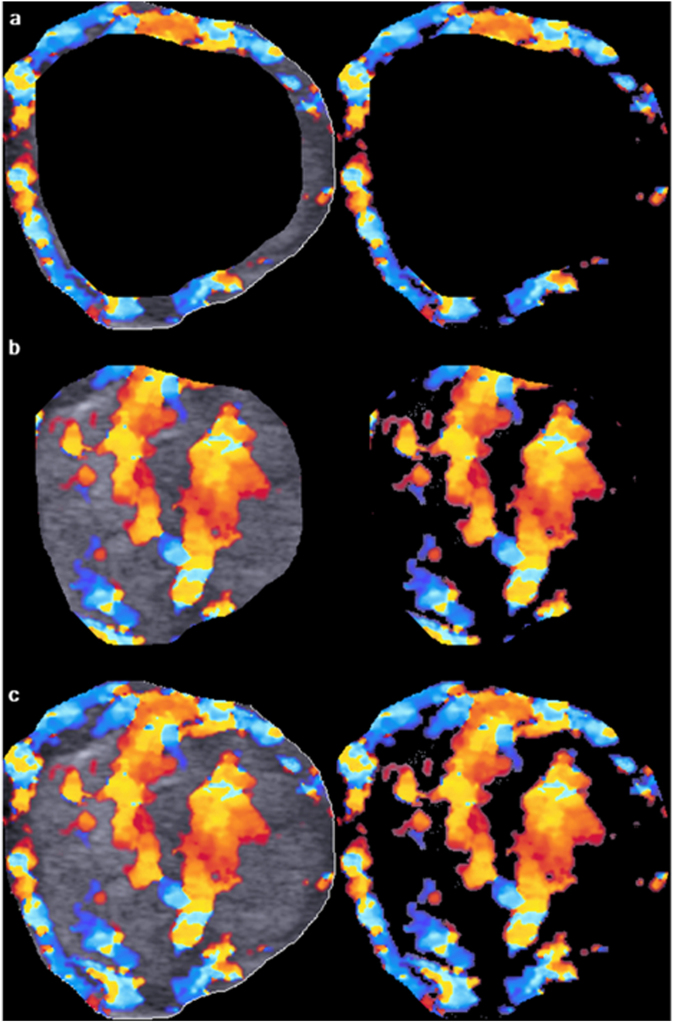
Color Doppler vascular index (VI) was assessed alone and in combination with grey-scale ultrasound (GSU) in regionally subdivided thyroid nodules in diagnosing thyroid cancer. Color Doppler sonograms of 111 thyroid nodules were evaluated by a home-developed algorithm that performed "offsetting" (algorithm for changing the area of a region of interest, ROI, without distorting the ROI's contour) and assessed peripheral, central and overall VI of thyroid nodules. Results showed that the optimum offset for dividing peripheral and central regions of nodule was 22%. At the optimum offset, the mean VI of peripheral, central, and overall regions of malignant nodules were significantly higher than those of benign nodules (26.5 ± 16.2%, 21.7 ± 19.6%, 23.8 ± 4.6% v/s 18.2 ± 16.7%, 11.9 ± 15.1% and 16.6 ± 1.8% respectively, P < 0.05). The optimum cut-off of peripheral, central, and overall VI was 19.7%, 9.1% and 20.2% respectively. When compared to GSU alone, combination of VI assessment with GSU evaluation of thyroid nodules increased the diagnostic accuracy from 58.6% to 79.3% (P < 0.05). In conclusion, a novel algorithm for regional subdivision and quantification of thyroid nodular VI in ultrasound images was established, and the optimum offset and cut-off were derived. Assessment of intranodular VI in conjunction with GSU can increase the accuracy in ultrasound diagnosis of thyroid cancer.
彩色多普勒血管指数(VI)单独评估和与灰阶超声(GSU)联合在区域性细分甲状腺结节中诊断甲状腺癌。使用自主开发的算法评估了 111 个甲状腺结节的彩色多普勒超声图像,该算法执行了“偏移”(改变感兴趣区域(ROI)面积而不改变 ROI 轮廓的算法),并评估了甲状腺结节的外周、中央和整体 VI。结果表明,用于划分结节外周和中央区域的最佳偏移量为 22%。在最佳偏移量下,恶性结节的外周、中央和整体区域的平均 VI 明显高于良性结节(26.5±16.2%、21.7±19.6%、23.8±4.6%比 18.2±16.7%、11.9±15.1%和 16.6±1.8%,P<0.05)。外周、中央和整体 VI 的最佳截断值分别为 19.7%、9.1%和 20.2%。与 GSU 单独评估相比,将 VI 评估与 GSU 评估甲状腺结节相结合,将诊断准确性从 58.6%提高到 79.3%(P<0.05)。总之,建立了一种新的超声图像甲状腺结节 VI 区域性细分和量化算法,并得出了最佳偏移量和截断值。联合 GSU 评估结节内 VI 可以提高甲状腺癌超声诊断的准确性。