Clinical Pharmacology, Bayer AG, Wuppertal, Germany.
Global Biostatistics, Bayer AG, Wuppertal, Germany.
Clin Pharmacokinet. 2018 Jun;57(6):647-661. doi: 10.1007/s40262-017-0604-7.
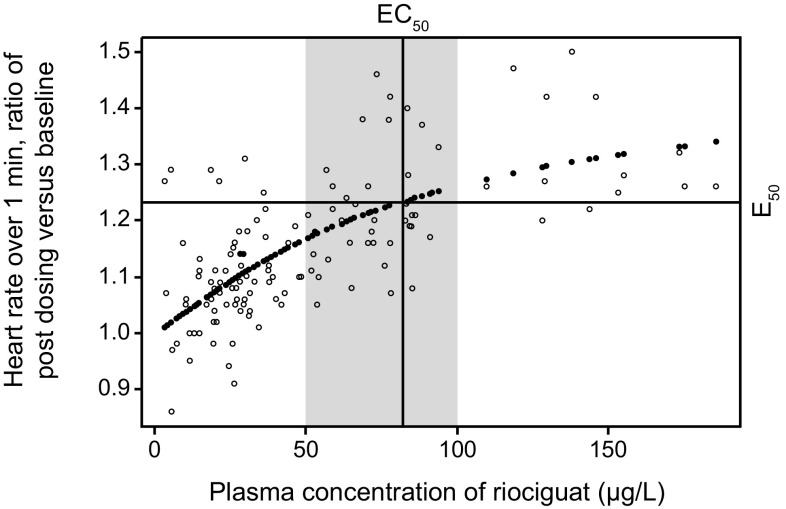
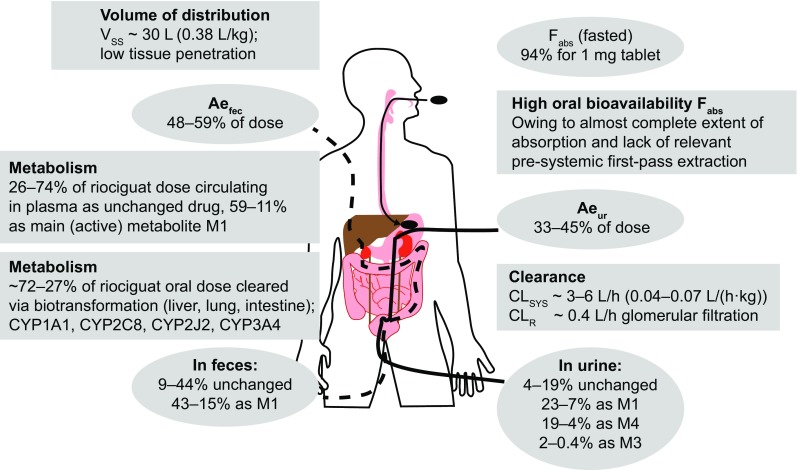
Oral riociguat is a soluble guanylate cyclase (sGC) stimulator that targets the nitric oxide (NO)-sGC-cyclic guanosine monophosphate pathway with a dual mode of action: directly by stimulating sGC, and indirectly by increasing the sensitivity of sGC to NO. It is rapidly absorbed, displays almost complete bioavailability (94.3%), and can be taken with or without food and as crushed or whole tablets. Riociguat exposure shows pronounced interindividual (60%) and low intraindividual (30%) variability in patients with pulmonary arterial hypertension (PAH) or chronic thromboembolic pulmonary hypertension (CTEPH), and is therefore administered using an individual dose-adjustment scheme at treatment initiation. The half-life of riociguat is approximately 12 h in patients and approximately 7 h in healthy individuals. Riociguat and its metabolites are excreted via both renal (33-45%) and biliary routes (48-59%), and dose adjustment should be performed with particular care in patients with moderate hepatic impairment or mild to severe renal impairment (no data exist for patients with severe hepatic impairment). The pharmacodynamic effects of riociguat reflect the action of a vasodilatory agent, and the hemodynamic response to riociguat correlated with riociguat exposure in patients with PAH or CTEPH in phase III population pharmacokinetic/pharmacodynamic analyses. Riociguat has a low risk of clinically relevant drug interactions due to its clearance by multiple cytochrome P450 (CYP) enzymes and its lack of effect on major CYP isoforms and transporter proteins at therapeutic levels. Riociguat has been approved for the treatment of PAH and CTEPH that is inoperable or persistent/recurrent after surgical treatment.
口服利奥西呱是一种可溶性鸟苷酸环化酶(sGC)刺激剂,其作用靶点为一氧化氮(NO)-sGC-环鸟苷酸途径,具有双重作用模式:直接刺激 sGC,间接增加 sGC 对 NO 的敏感性。它吸收迅速,几乎完全生物利用度(94.3%),可与食物同服或不服,可整片或碾碎服用。肺动脉高压(PAH)或慢性血栓栓塞性肺动脉高压(CTEPH)患者的利奥西呱暴露量存在明显的个体间(60%)和低个体内(30%)变异性,因此在治疗开始时采用个体化剂量调整方案进行给药。PAH 或 CTEPH 患者的利奥西呱半衰期约为 12 h,健康受试者约为 7 h。利奥西呱及其代谢物通过肾脏(33-45%)和胆道(48-59%)排泄,中重度肝损伤或轻至重度肾损伤患者(无重度肝损伤患者数据)应特别谨慎调整剂量。利奥西呱的药效学作用反映了血管扩张剂的作用,PAH 或 CTEPH 患者的 III 期群体药代动力学/药效学分析显示,利奥西呱的血流动力学反应与利奥西呱暴露量相关。由于其清除主要依赖多种细胞色素 P450(CYP)酶,且在治疗水平时对主要 CYP 同工酶和转运蛋白无影响,利奥西呱发生具有临床意义的药物相互作用的风险较低。利奥西呱已获批用于治疗不可手术或手术治疗后持续/复发的 PAH 和 CTEPH。