Györi Georg P, Felsenreich D Moritz, Silberhumer Gerd R, Soliman Thomas, Berlakovich Gabriela A
Department of Surgery, Division of Transplantation, Medical University of Vienna, Währinger Gürtel 18-20, 1090 Vienna, Austria.
Eur Surg. 2017;49(5):236-243. doi: 10.1007/s10353-017-0487-8. Epub 2017 Sep 4.
It is current practice that patients with hepatocellular carcinoma (HCC) listed for liver transplantation should receive locoregional treatment if the suspected waiting time for transplantation is longer than 6 months, even in the absence of prospective randomized data. Aim of this study was the comparison of single versus multimodality locoregional treatment strategies on outcomes after liver transplantation.
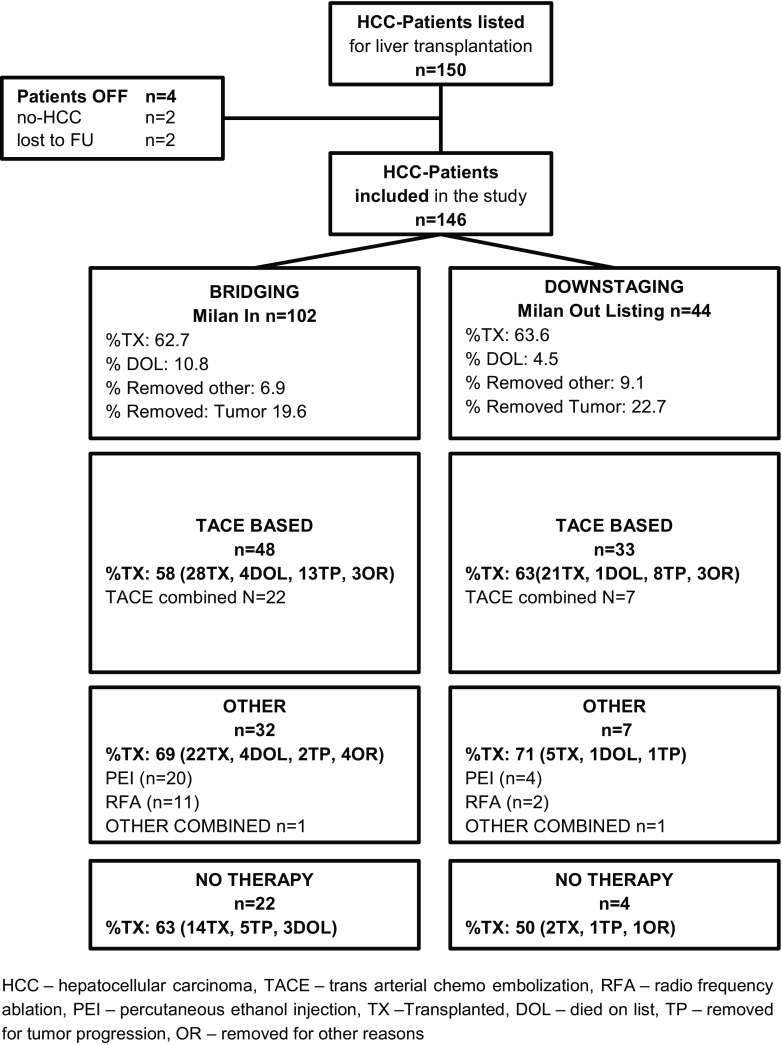
This is a retrospective analysis of 150 HCC patients listed for liver transplantation at our center between 2004 and 2011. Outcomes were analyzed according to modified Response Evaluation Criteria in Solid Tumors (mRECIST) in relation to intention-to-treat and overall survival after liver transplantation.
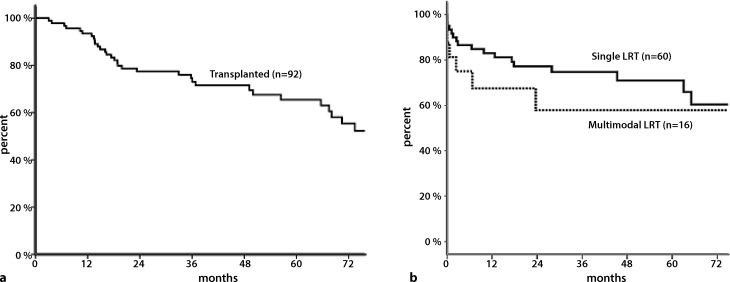
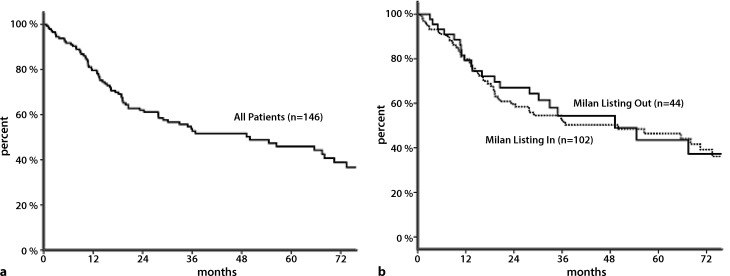
Overall, 92 patients (63%) were transplanted in this cohort. The intention-to-treat 1‑, 3‑, 5‑year waiting list survival was 80, 59, and 50% respectively. In RFA-(radiofrequency ablative) and TACE-(transarterial chemoembolisation)-based regimens, rates of transplanted patients were comparable (69 vs. 58%, = ns). No difference was seen in overall survival after liver transplantation when comparing TACE- and RFA-based regimens. Patients receiving multimodality locoregional therapy had lower overall survival after transplantation ( = 0.05).
TACE- and RFA-based regimens showed equal outcomes in terms of transplantation rate, tumor response, and post-transplant survival. Patients in need of more than one treatment modality might identify a cohort with poorer post-transplant survival.
Direct comparison of TACE and RFA in a multimodality setting, analysis according to mRECIST.
目前的做法是,列入肝移植名单的肝细胞癌(HCC)患者,如果预计等待移植的时间超过6个月,即使缺乏前瞻性随机数据,也应接受局部区域治疗。本研究的目的是比较单模式与多模式局部区域治疗策略对肝移植后结局的影响。
这是一项对2004年至2011年间在本中心列入肝移植名单的150例HCC患者的回顾性分析。根据改良实体瘤疗效评价标准(mRECIST)分析肝移植后的意向性治疗和总生存结局。
总体而言,该队列中有92例(63%)患者接受了移植。意向性治疗的1年、3年、5年等待名单生存率分别为80%、59%和50%。在基于射频消融(RFA)和经动脉化疗栓塞(TACE)的治疗方案中,移植患者的比例相当(69%对58%,P=无显著性差异)。比较基于TACE和RFA的治疗方案时,肝移植后的总生存无差异。接受多模式局部区域治疗的患者移植后的总生存较低(P=0.05)。
基于TACE和RFA的治疗方案在移植率、肿瘤反应和移植后生存方面显示出相同的结局。需要不止一种治疗模式的患者可能属于移植后生存较差的队列。
在多模式背景下直接比较TACE和RFA,根据mRECIST进行分析。