Boles U, Gul E E, Fitzgerald L, Sadiq Ali F, Nolan C, Aldworth-Gaumond K, Redfearn D R, Baranchuk A, Glover B, Simpson C, Abdollah H, Michael K A
Heart Rhythm Service, Division of Cardiology, Kingston General Hospital, Queen's University, Ontario, Canada; Cardiology Department, Midland Regional Hospital Mullingar (MRHM), Ireland.
Heart Rhythm Service, Division of Cardiology, Kingston General Hospital, Queen's University, Ontario, Canada.
Indian Pacing Electrophysiol J. 2018 Mar-Apr;18(2):56-60. doi: 10.1016/j.ipej.2017.10.010. Epub 2017 Oct 27.
Current algorithms and device morphology templates have been proposed in current Implantable Cardioverter-Defibrillators (ICDs) to minimize inappropriate therapies (ITS), but this has not been completely successful.
Assess the impact of a deliberate strategy of using an atrial lead implant with standardized parameters; based on all current ICD discriminators and technologies, on the burden of ITS.
A retrospective single-centre analysis of 250 patients with either dual chamber (DR) ICDs or biventricular ICDs (CRTDs) over a (41.9 ± 27.3) month period was performed. The incidence of ITS on all ICD and CRTD patients was chronicled after the implementation of standardized programming.
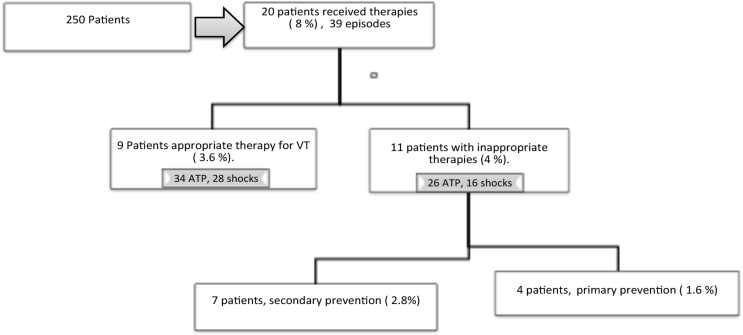
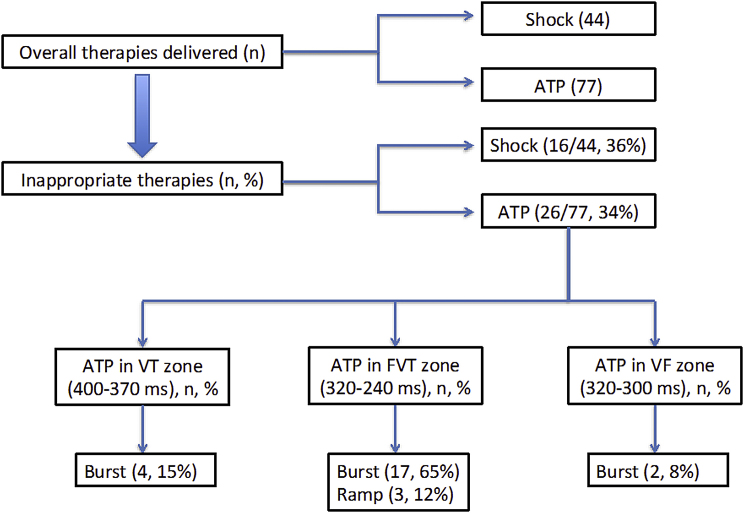
39 events of anti-tachycardial pacing (ATP) and/or shocks were identified in 20 patients (8% incidence rate among patients). The total number of individual therapies was 120, of which 34% were inappropriate ATP, and 36% were inappropriate shocks. 11 patients of the 250 patients received ITS (4.4%). Of the 20 patients, four had ICDs for primary prevention and 16 for a secondary prevention. All the episodes in the primary indication group were inappropriate, while seven patients (43%) of the secondary indication group experienced inappropriate therapies.
The burden of ITS in the population of patients receiving ICDs was 4.4% in the presence of atrial leads. The proposed rationalized programming criteria seems an effective strategy to minimize the burden of inappropriate therapies and will require further validation.
目前已在植入式心脏转复除颤器(ICD)中提出了当前算法和设备形态模板,以尽量减少不适当治疗(ITS),但这尚未完全成功。
评估采用标准化参数进行心房导线植入的刻意策略;基于所有当前的ICD鉴别器和技术,对ITS负担的影响。
对250例双腔(DR)ICD或双心室ICD(CRTD)患者进行了为期(41.9±27.3)个月的回顾性单中心分析。在实施标准化编程后,记录了所有ICD和CRTD患者的ITS发生率。
在20例患者中识别出39次抗心动过速起搏(ATP)和/或电击事件(患者发生率为8%)。个体治疗总数为120次,其中34%为不适当的ATP,36%为不适当的电击。250例患者中有11例接受了ITS(4.4%)。在这20例患者中,4例因一级预防植入ICD,16例因二级预防植入。一级适应证组的所有发作均不适当;而二级适应证组中有7例患者(43%)经历了不适当治疗。
在有心房导线的情况下,接受ICD治疗的患者群体中ITS负担为4.4%。所提出的合理化编程标准似乎是一种有效策略,可尽量减少不适当治疗的负担,且需要进一步验证。