Department of Laboratory Medicine, San Francisco Medical Center, University of California, San Francisco.
Department of Pathology and Laboratory Medicine, West Connecticut Healthcare Network, Danbury Hospital Campus, Danbury, CT.
Am J Surg Pathol. 2018 Feb;42(2):269-276. doi: 10.1097/PAS.0000000000000982.
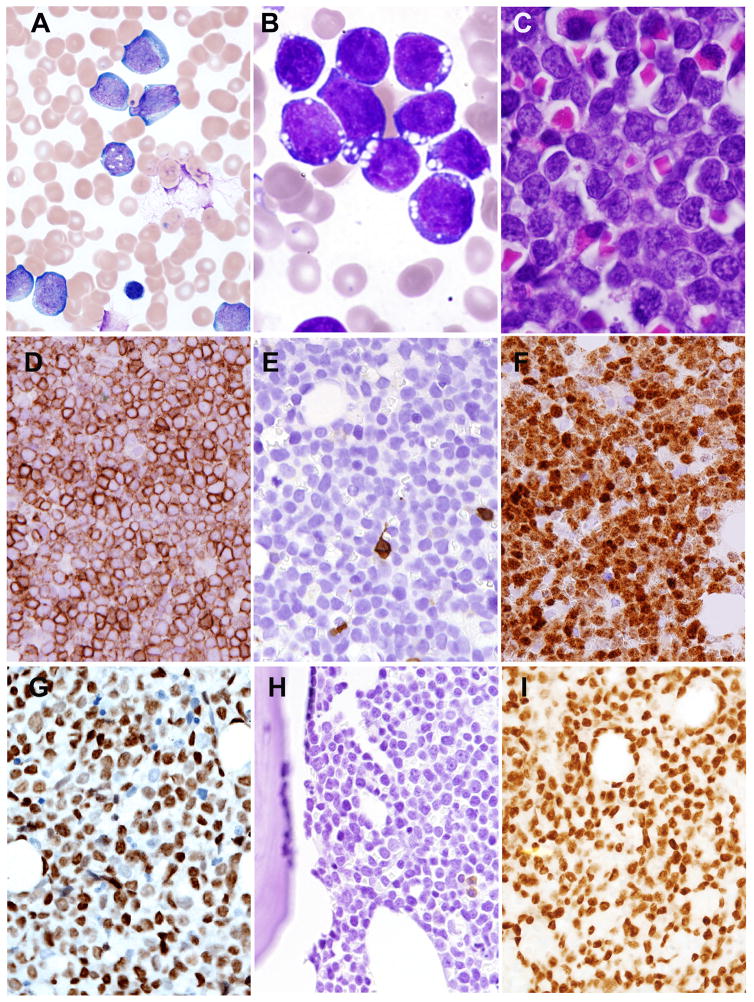
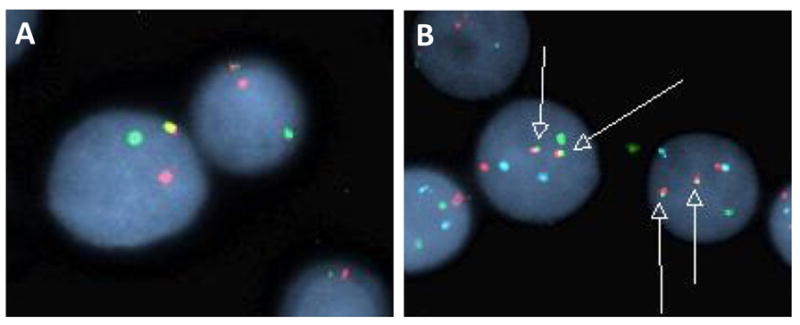
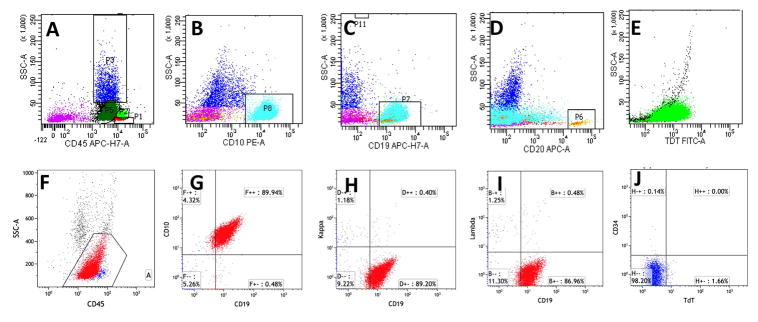
Isolated MYC rearrangement without other recurrent genetic abnormalities is rare in B lymphoblastic leukemia/lymphoma (B-ALL/LBL), with most cases reported in pediatric patients. We report 3 adult cases with lymphoblasts showing a precursor B cell immunophenotype, and isolated MYC/IGH translocation. All 3 cases occurred in male patients with initial presentation of diffuse lymphadenopathy. Cases 1 and 2 had B-ALL with significantly increased lymphoblasts in peripheral blood and bone marrow. Case 3, a patient with human immunodeficiency virus infection, had the diagnosis of B-LBL made on a retroperitoneal lymph node biopsy and had no peripheral blood or bone marrow involvement. The leukemic and lymphoma cells in all 3 cases demonstrated Burkitt lymphoma-like morphology with deeply basophilic cytoplasm and numerous cytoplasmic vacuoles. However, all 3 had immature immunophenotypes including expression of terminal deoxynucleotidyl transferase (TdT), absence of BCL6, and dim-to-negative CD45. CD20 was largely negative in 2 of 3 cases. All 3 had confirmed MYC/IGH translocation, but lacked rearrangements of BCL2 or BCL6. EBV was negative by Epstein-Barr virus encoded small RNA in situ hybridization. Treatment protocols varied, including both high-risk ALL-type (protocol 8707) and high-grade lymphoma regimens (hyper-CVAD [cyclophosphamide, vincristine, adriamycin, and dexamethasone]), but no patient achieved continuous complete remission. These cases seem to represent a distinct biological phenomenon, in which a MYC translocation may be acquired at an immature stage of differentiation, thus manifesting features of both B-ALL/LBL and Burkitt lymphoma.
孤立性 MYC 重排而无其他常见遗传异常的情况在 B 淋巴母细胞白血病/淋巴瘤(B-ALL/LBL)中较为罕见,且大多数报道见于儿科患者。我们报告了 3 例成人病例,这些病例的淋巴母细胞表现出前体 B 细胞免疫表型,且存在孤立性 MYC/IGH 易位。所有 3 例均发生于男性患者,初始表现为弥漫性淋巴结病。病例 1 和 2 为 B-ALL,外周血和骨髓中显著增加了淋巴母细胞。病例 3 为人类免疫缺陷病毒感染患者,在腹膜后淋巴结活检时诊断为 B-LBL,且无外周血或骨髓受累。所有 3 例的白血病和淋巴瘤细胞均表现出伯基特淋巴瘤样形态,具有深嗜碱性细胞质和大量细胞质空泡。然而,所有 3 例均具有不成熟的免疫表型,包括末端脱氧核苷酸转移酶(TdT)表达、BCL6 缺失以及 CD45 弱至阴性。3 例中有 2 例 CD20 大部分阴性。所有 3 例均证实存在 MYC/IGH 易位,但缺乏 BCL2 或 BCL6 重排。通过 Epstein-Barr 病毒编码的小 RNA 原位杂交检测 EBV 为阴性。治疗方案各不相同,包括高危 ALL 型(方案 8707)和高级别淋巴瘤方案(高剂量环磷酰胺、长春新碱、多柔比星和地塞米松),但没有患者获得持续完全缓解。这些病例似乎代表了一种独特的生物学现象,其中 MYC 易位可能在分化的不成熟阶段获得,从而表现出 B-ALL/LBL 和伯基特淋巴瘤的特征。