Cagle Laura A, Franzi Lisa M, Linderholm Angela L, Last Jerold A, Adams Jason Y, Harper Richart W, Kenyon Nicholas J
Center for Comparative Respiratory Biology and Medicine, University of California, Davis, Davis, CA, United States of America.
Division of Pulmonary, Critical Care, and Sleep Medicine, School of Medicine, University of California, Davis, Davis, CA, United States of America.
PLoS One. 2017 Nov 7;12(11):e0187419. doi: 10.1371/journal.pone.0187419. eCollection 2017.
Positive-pressure mechanical ventilation is an essential therapeutic intervention, yet it causes the clinical syndrome known as ventilator-induced lung injury. Various lung protective mechanical ventilation strategies have attempted to reduce or prevent ventilator-induced lung injury but few modalities have proven effective. A model that isolates the contribution of mechanical ventilation on the development of acute lung injury is needed to better understand biologic mechanisms that lead to ventilator-induced lung injury.
To evaluate the effects of positive end-expiratory pressure and recruitment maneuvers in reducing lung injury in a ventilator-induced lung injury murine model in short- and longer-term ventilation.
5-12 week-old female BALB/c mice (n = 85) were anesthetized, placed on mechanical ventilation for either 2 hrs or 4 hrs with either low tidal volume (8 ml/kg) or high tidal volume (15 ml/kg) with or without positive end-expiratory pressure and recruitment maneuvers.
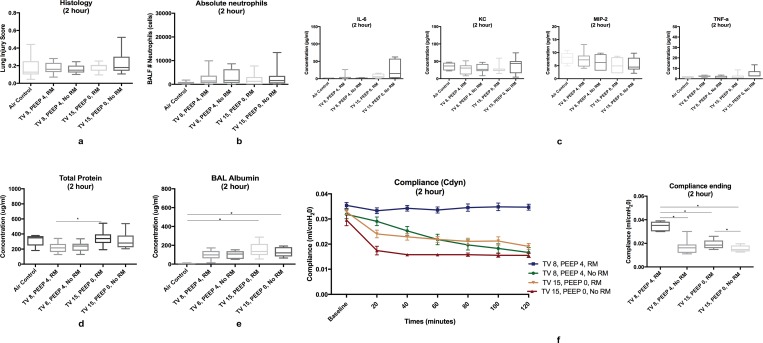
Alteration of the alveolar-capillary barrier was noted at 2 hrs of high tidal volume ventilation. Standardized histology scores, influx of bronchoalveolar lavage albumin, proinflammatory cytokines, and absolute neutrophils were significantly higher in the high-tidal volume ventilation group at 4 hours of ventilation. Application of positive end-expiratory pressure resulted in significantly decreased standardized histology scores and bronchoalveolar absolute neutrophil counts at low- and high-tidal volume ventilation, respectively. Recruitment maneuvers were essential to maintain pulmonary compliance at both 2 and 4 hrs of ventilation.
Signs of ventilator-induced lung injury are evident soon after high tidal volume ventilation (as early as 2 hours) and lung injury worsens with longer-term ventilation (4 hrs). Application of positive end-expiratory pressure and recruitment maneuvers are protective against worsening VILI across all time points. Dynamic compliance can be used guide the frequency of recruitment maneuvers to help ameloriate ventilator-induced lung injury.
正压机械通气是一项重要的治疗干预措施,但它会引发被称为呼吸机诱导性肺损伤的临床综合征。各种肺保护性机械通气策略都试图减少或预防呼吸机诱导性肺损伤,但很少有方法被证明有效。需要一个能够分离机械通气对急性肺损伤发展的影响的模型,以便更好地理解导致呼吸机诱导性肺损伤的生物学机制。
评估在短期和长期通气的呼吸机诱导性肺损伤小鼠模型中,呼气末正压和肺复张手法在减轻肺损伤方面的效果。
将85只5至12周龄的雌性BALB/c小鼠麻醉,分别采用低潮气量(8毫升/千克)或高潮气量(15毫升/千克)进行2小时或4小时的机械通气,通气过程中或有或无呼气末正压和肺复张手法。
在高潮气量通气2小时时,肺泡-毛细血管屏障出现改变。通气4小时时,高潮气量通气组的标准化组织学评分、支气管肺泡灌洗白蛋白流入量、促炎细胞因子和绝对中性粒细胞数均显著更高。在低潮气量和高潮气量通气时,应用呼气末正压分别使标准化组织学评分和支气管肺泡绝对中性粒细胞计数显著降低。肺复张手法对于在通气2小时和4小时时维持肺顺应性至关重要。
高潮气量通气后不久(最早2小时),呼吸机诱导性肺损伤的迹象就很明显,且随着长期通气(4小时)肺损伤会恶化。在所有时间点,应用呼气末正压和肺复张手法都可防止呼吸机诱导性肺损伤恶化。动态顺应性可用于指导肺复张手法的频率,以帮助改善呼吸机诱导性肺损伤。