Yamei Wu, Rongmu Luo, Yongbin Cao, Yingjian Si, Xiaohong Li, Xiaomei Zhang, Pei Yan, Zhenlan Du, Haitao Wang, Jing Wang, Bojing Wang, Xiaoxiong Wu, Wanming Da
Department of Hematology, The First Affiliated Hospital, Chinese PLA General Hospital, Beijing 100048, China.
Department of Hematology, Affiliated BaYi Children's Hospital, PLA Army General Hospital, Beijing 100700, China.
Oncotarget. 2017 Jul 31;8(48):83817-83830. doi: 10.18632/oncotarget.19745. eCollection 2017 Oct 13.
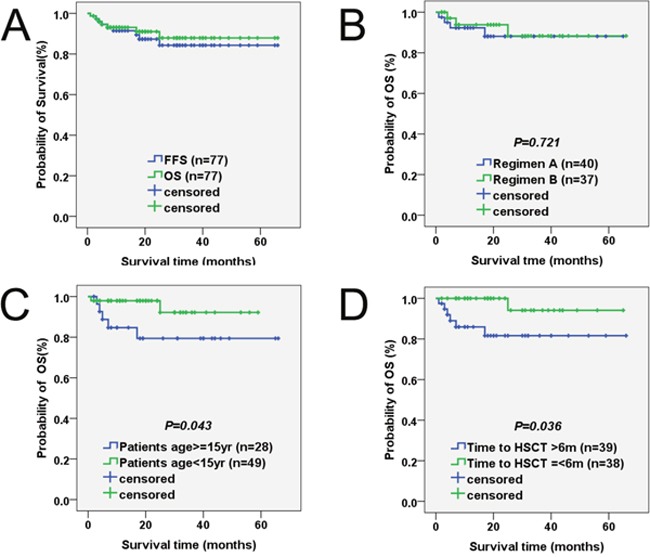
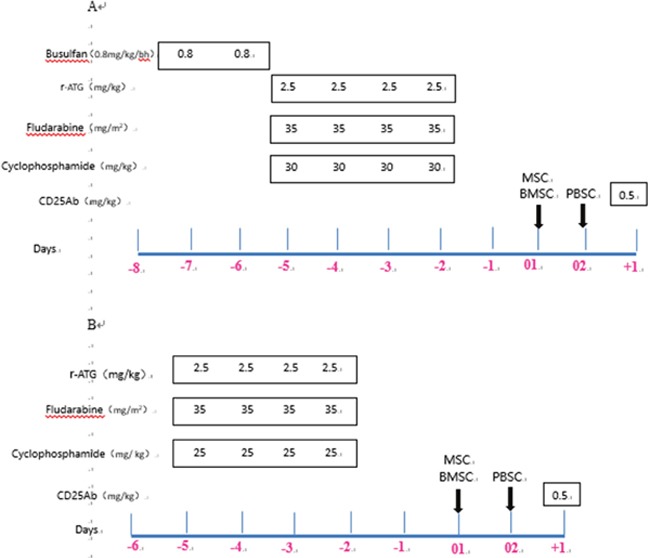
Significant improvements in hematopoietic stem cell transplantation (HSCT) with haploidentical family donors (HFD) have confirmed its therapeutic role in severe aplastic anemia (SAA) and led to the evolution of treatment algorithms. However, the optimal conditioning regimen for HFD-HSCT remains undefined, especially the dosage of cyclophosphamide (Cy). A total of 77 patients with SAA from two research centers, who received HFD-HSCT with reduced-intensity fludarabine + cyclophosphamide + thymoglobulin ± busulfan conditioning regimen plus third-party cells infusion were included in this study, of which 67 pairs had 4-5 loci mismatched. We were particularly interested in whether the dosage of Cy significantly impacted graft failure (GF) and overall survival (OS). All patients showed sustained hematopoietic engraftment without any increase in severe aGVHD and transplantation-related mortality (TRM). The incidences of grade II-IV aGVHD, grade III-IV aGVHD and extensive cGVHD were 18%, 10% and 7%, respectively. The probabilities of 1-year and 5-year OS were 93.1% and 87.9%, respectively. Furthermore, patient age <15 years, MNC cells >8×10/kg and donor age <45 years were associated with better survival (=0.043, =0.023, and =0.037, respectively) and engraftment (=0.019, =0.008, and =0.001, respectively). Our findings indicated that SAA patients lack MSD benefited the most if HFD-HSCT was performed with reduced-intensity fludarabine-based conditioning regimen. Improved outcomes with HFD-HSCT may lead to a salvaged therapy and an expanded direct role for SAA in the future.
单倍体相合家庭供者造血干细胞移植(HFD-HSCT)取得的显著进展证实了其在重型再生障碍性贫血(SAA)中的治疗作用,并推动了治疗方案的演变。然而,HFD-HSCT的最佳预处理方案仍不明确,尤其是环磷酰胺(Cy)的剂量。本研究纳入了来自两个研究中心的77例接受HFD-HSCT的SAA患者,采用氟达拉滨+环磷酰胺+抗胸腺细胞球蛋白±白消安减低强度预处理方案并输注第三方细胞,其中67对存在4-5个位点错配。我们特别关注Cy剂量是否会显著影响移植物失败(GF)和总生存期(OS)。所有患者均实现了持续造血植入,且重度急性移植物抗宿主病(aGVHD)和移植相关死亡率(TRM)均未增加。II-IV级aGVHD、III-IV级aGVHD和广泛性慢性移植物抗宿主病(cGVHD)的发生率分别为18%、10%和7%。1年和5年OS概率分别为93.1%和87.9%。此外,患者年龄<15岁、单个核细胞(MNC)>8×10/kg和供者年龄<45岁与更好的生存(分别为=0.043、=0.023和=0.037)及植入(分别为=0.019、=0.008和=0.001)相关。我们的研究结果表明,对于缺乏同胞全相合供者(MSD)的SAA患者,采用基于氟达拉滨的减低强度预处理方案进行HFD-HSCT获益最大。HFD-HSCT改善的疗效可能会带来挽救性治疗,并在未来扩大SAA的直接治疗作用。