Institute for Medical Informatics, Biometry and Epidemiology, University Duisburg-Essen, Germany (N.L. R.E., S. Moebus, A.S., U.R., K.-H.J.)
Institute for Medical Informatics, Biometry and Epidemiology, University Duisburg-Essen, Germany (N.L. R.E., S. Moebus, A.S., U.R., K.-H.J.).
Circulation. 2018 Feb 13;137(7):665-679. doi: 10.1161/CIRCULATIONAHA.116.027034. Epub 2017 Nov 15.
Computed tomography (CT) allows estimation of coronary artery calcium (CAC) progression. We evaluated several progression algorithms in our unselected, population-based cohort for risk prediction of coronary and cardiovascular events.
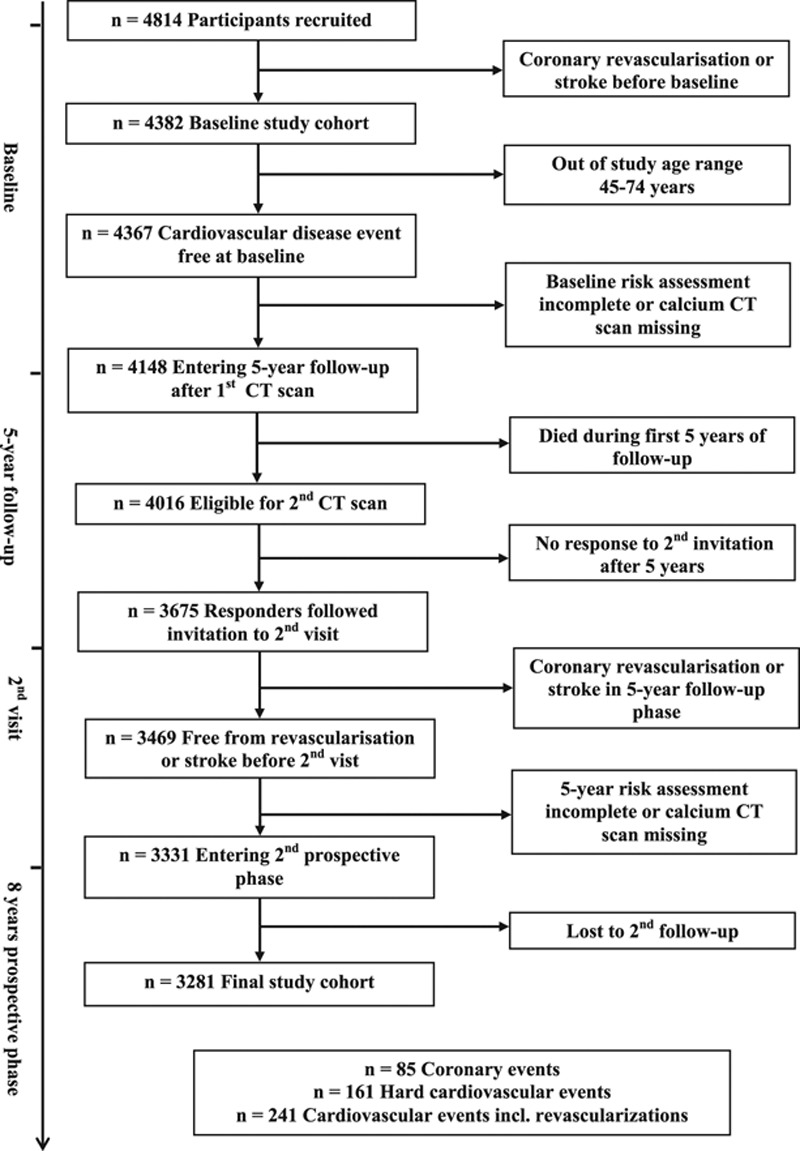
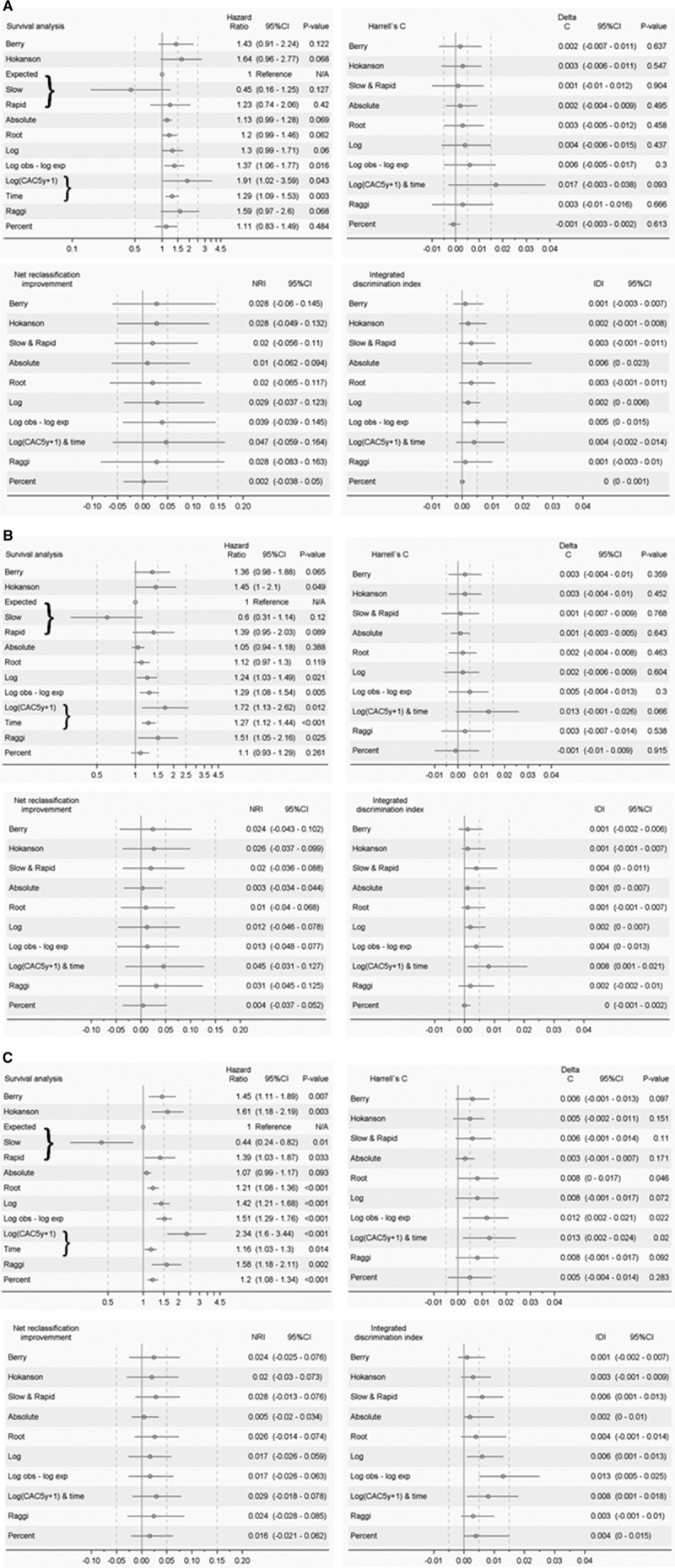
In 3281 participants (45-74 years of age), free from cardiovascular disease until the second visit, risk factors, and CTs at baseline (b) and after a mean of 5.1 years (5y) were measured. Hard coronary and cardiovascular events, and total cardiovascular events including revascularization, as well, were recorded during a follow-up time of 7.8±2.2 years after the second CT. The added predictive value of 10 CAC progression algorithms on top of risk factors including baseline CAC was evaluated by using survival analysis, C-statistics, net reclassification improvement, and integrated discrimination index. A subgroup analysis of risk in CAC categories was performed.
We observed 85 (2.6%) hard coronary, 161 (4.9%) hard cardiovascular, and 241 (7.3%) total cardiovascular events. Absolute CAC progression was higher with versus without subsequent coronary events (median, 115 [Q1-Q3, 23-360] versus 8 [0-83], <0.0001; similar for hard/total cardiovascular events). Some progression algorithms added to the predictive value of baseline CT and risk assessment in terms of C-statistic or integrated discrimination index, especially for total cardiovascular events. However, CAC progression did not improve models including CAC and 5-year risk factors. An excellent prognosis was found for 921 participants with double-zero CAC=CAC=0 (10-year coronary and hard/total cardiovascular risk: 1.4%, 2.0%, and 2.8%), which was for participants with incident CAC 1.8%, 3.8%, and 6.6%, respectively. When CAC progressed from 1 to 399 to CAC≥400, coronary and total cardiovascular risk were nearly 2-fold in comparison with subjects who remained below CAC=400. Participants with CAC≥400 had high rates of hard coronary and hard/total cardiovascular events (10-year risk: 12.0%, 13.5%, and 30.9%, respectively).
CAC progression is associated with coronary and cardiovascular event rates, but adds only weakly to risk prediction. What counts is the most recent CAC value and risk factor assessment. Therefore, a repeat scan >5 years after the first scan may be of additional value, except when a double-zero CT scan is present or when the subjects are already at high risk.
计算机断层扫描(CT)可用于估计冠状动脉钙(CAC)的进展。我们在未选择的、基于人群的队列中评估了几种进展算法,用于预测冠状动脉和心血管事件的风险。
在 3281 名参与者(45-74 岁)中,在第二次就诊前没有心血管疾病,危险因素和基线(b)和平均 5.1 年后(5y)的 CT 均有测量。在第二次 CT 后 7.8±2.2 年的随访期间,记录了硬冠状动脉和心血管事件以及包括血运重建在内的总心血管事件。通过生存分析、C 统计量、净重新分类改善和综合判别指数,评估了 10 种 CAC 进展算法在包括基线 CAC 在内的危险因素之上的附加预测价值。对 CAC 分类风险的亚组分析。
我们观察到 85 例(2.6%)硬冠状动脉、161 例(4.9%)硬心血管和 241 例(7.3%)总心血管事件。与无后续冠状动脉事件相比,有事件者的 CAC 绝对进展更高(中位数,115[Q1-Q3,23-360]与 8[0-83],<0.0001;硬/总心血管事件类似)。某些进展算法在 C 统计量或综合判别指数方面增加了基线 CT 和风险评估的预测价值,特别是对总心血管事件。然而,CAC 进展并未改善包括 CAC 和 5 年风险因素的模型。对于 CAC=CAC=0 的 921 名双零参与者(10 年冠状动脉和硬/总心血管风险:1.4%、2.0%和 2.8%),预后极好,而 CAC 为 1 至 399 的参与者为 1.8%、3.8%和 6.6%,分别为 400。当 CAC 从 1 增加到 399 增加到 CAC≥400 时,与 CAC≤400 的受试者相比,冠状动脉和总心血管风险几乎增加了一倍。CAC≥400 的患者硬冠状动脉和硬/总心血管事件的发生率较高(10 年风险:12.0%、13.5%和 30.9%)。
CAC 进展与冠状动脉和心血管事件的发生率相关,但对风险预测的贡献较弱。重要的是最近的 CAC 值和风险因素评估。因此,除了第一次扫描后 5 年以上的重复扫描可能具有附加价值之外,当出现双零 CT 扫描或患者已经处于高风险时,这种扫描可能没有附加价值。