Huang Chao-Min, Hu Tsung-Hui, Chang Kuo-Chin, Tseng Po-Lin, Lu Sheng-Nan, Chen Chien-Hung, Wang Jing-Houng, Lee Chuan-Mo, Tsai Ming-Chao, Lin Ming-Tsung, Yen Yi-Hao, Hung Chao-Hung, Cho Chung-Lung, Wu Cheng-Kun
aDepartment of Biological Sciences, National Sun Yat-Sen University bDivision of Hepatogastroenterology, Department of Internal Medicine, Kaohsiung Chang Gung Memorial Hospital and Chang Gung University College of Medicine, Kaohsiung, Taiwan.
Medicine (Baltimore). 2017 Nov;96(46):e8696. doi: 10.1097/MD.0000000000008696.
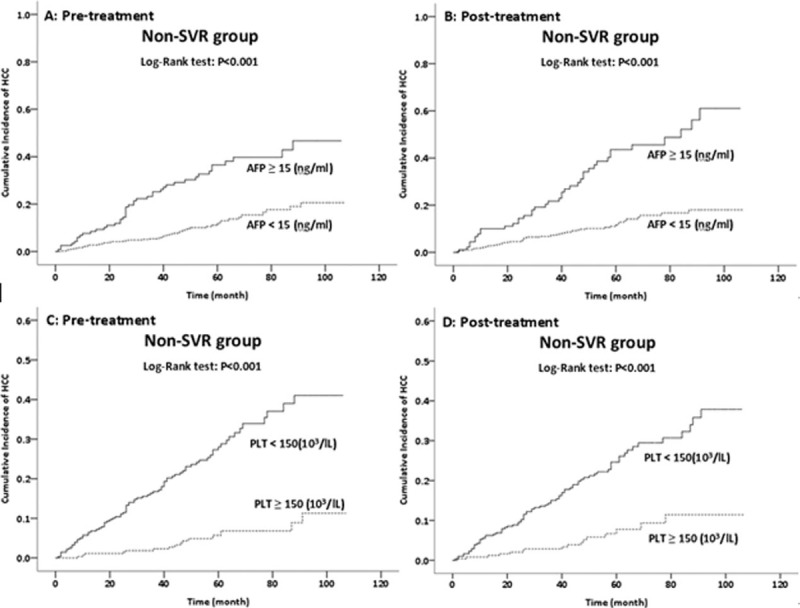
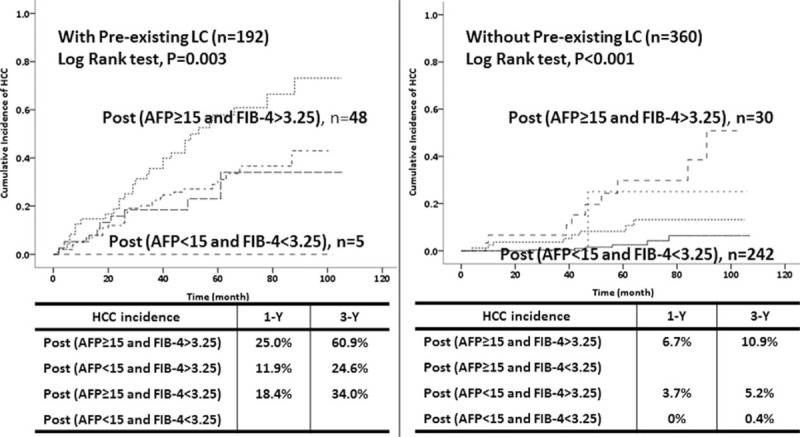
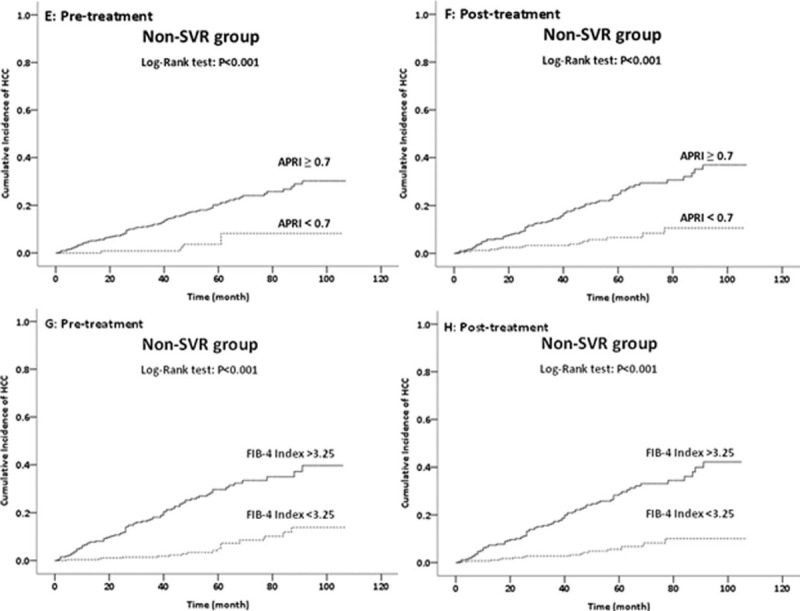
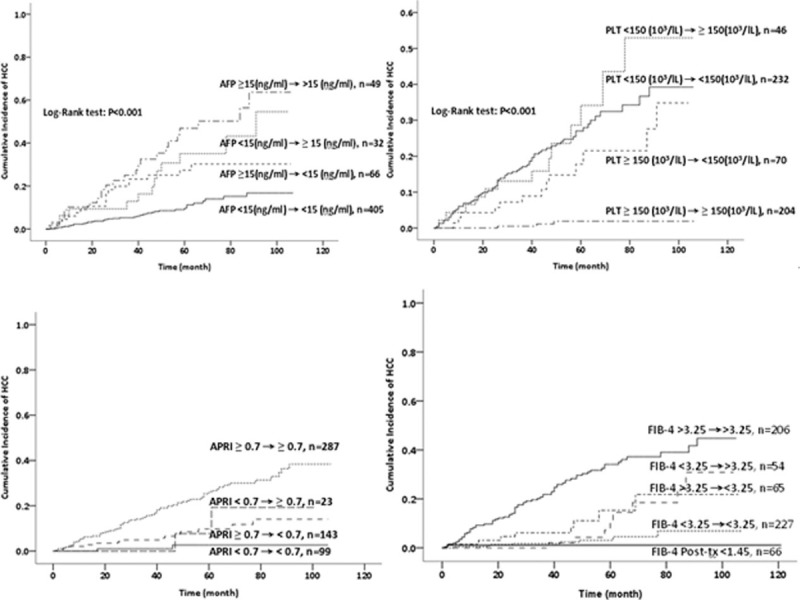
Some patients with hepatitis C virus (HCV) infections who fail to achieve sustained virological responses (SVRs) after interferon (IFN) therapy do not develop hepatocellular carcinoma (HCC). Risk stratification of these patients may help identify those who would benefit most from treatment with direct-acting antivirals (DAAs).A total of 552 HCV-infected patients with non-SVR status were enrolled. Laboratory data before and after IFN treatment were analyzed to determine the relationship of changes in serum markers with development of HCC during the 7-year study period.HCC developed in 93 patients. The risk factors for HCC were pre-existing liver cirrhosis, low hemoglobin level at baseline, low pretreatment platelet count, high post-treatment alpha-fetoprotein (AFP) level (≥15 ng/mL), and high post-treatment Fibrosis 4 (FIB4) index (>3.25). For patients without pre-existing cirrhosis, those with high post-treatment AFP level and FIB4 index had the highest risk of HCC (1 year: 6.7%; 3 years: 10.9%; 5 years: 29.7%), followed by those with high post-treatment AFP level and low post-treatment FIB4 index (5 years: 25%), and those with low post-treatment AFP level and high post-treatment FIB4 index (1 year: 3.7%; 3 years: 5.2%; 5 years: 10.6%). The risk was even lower for patients with low post-treatment AFP level and FIB4 index (1 year: 0%; 3 years: 0.4%; 5 years: 2.5%). None of the patients with FIB4 indexes consistently below 1.45 developed HCC.The combined use of post-treatment AFP level and FIB4 index was useful for risk stratification of HCV-infected patients with non-SVR status after IFN therapy. These data may help clinicians to identify patients who most urgently need DAA treatment.
一些丙型肝炎病毒(HCV)感染患者在接受干扰素(IFN)治疗后未实现持续病毒学应答(SVR),但未发生肝细胞癌(HCC)。对这些患者进行风险分层可能有助于识别那些最能从直接抗病毒药物(DAA)治疗中获益的患者。
共纳入了552例非SVR状态的HCV感染患者。分析IFN治疗前后的实验室数据,以确定血清标志物变化与7年研究期间HCC发生之间的关系。
93例患者发生了HCC。HCC的危险因素包括既往存在肝硬化、基线血红蛋白水平低、治疗前血小板计数低、治疗后甲胎蛋白(AFP)水平高(≥15 ng/mL)以及治疗后纤维化4(FIB4)指数高(>3.25)。对于无既往肝硬化的患者,治疗后AFP水平高且FIB4指数高的患者发生HCC的风险最高(1年:6.7%;3年:10.9%;5年:29.7%),其次是治疗后AFP水平高且治疗后FIB4指数低的患者(5年:25%),以及治疗后AFP水平低且治疗后FIB4指数高的患者(1年:3.7%;3年:5.2%;5年:10.6%)。治疗后AFP水平低且FIB4指数低的患者风险更低(1年:0%;3年:0.4%;5年:2.5%)。FIB4指数持续低于1.45的患者均未发生HCC。
治疗后AFP水平和FIB4指数联合应用有助于对IFN治疗后非SVR状态的HCV感染患者进行风险分层。这些数据可能有助于临床医生识别最急需DAA治疗的患者。