Yu Mi-Yeon, Kim Yong-Chul, Koo Ho Suk, Chin Ho Jun
Department of Internal Medicine, Seoul National University Hospital, Seoul, Korea.
Department of Internal Medicine, Inje University Seoul Paik Hospital, Seoul, Korea.
PLoS One. 2017 Nov 20;12(11):e0188375. doi: 10.1371/journal.pone.0188375. eCollection 2017.
The immunosuppressive drug tacrolimus has the short-term effect of reducing proteinuria in patients with immunoglobulin A nephropathy (IgAN). Our study investigated the effects on proteinuria and kidney function after discontinuation of tacrolimus.
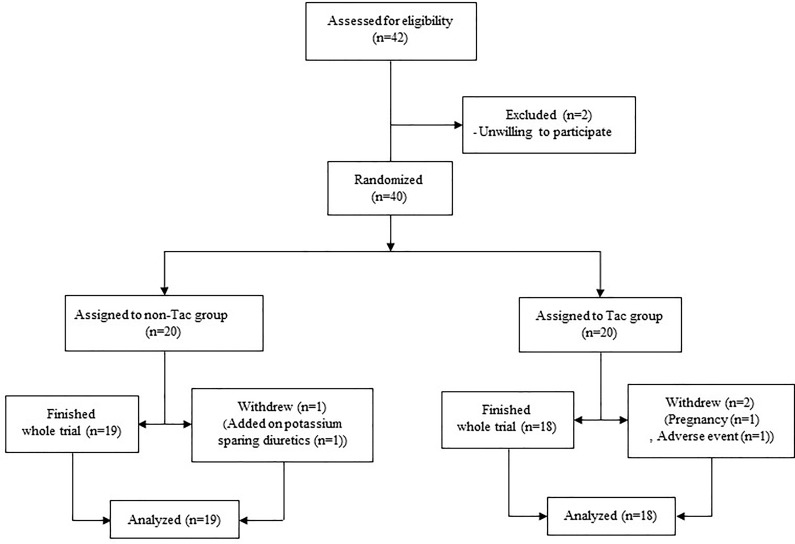
Patients with biopsy-proven IgAN were included in the study and randomly divided into two treatment groups. There was a corresponding control group for each treatment group. The first group included patients treated with tacrolimus (Tac vs non-Tac group) and the second group included patients with a renin angiotensin system blocker (RASi vs non-RASi group). The Tac group received treatment for up to 16 weeks, with the administration of tacrolimus being ceased at the final visit (trial phase). We tracked the patients at 12, 24, 52, and 240 weeks (observational phase). The primary outcomes examined were the percentage change (from the trial phase to the observational phase) of time-averaged proteinuria (TA-proteinuria; g/g creatinine [cr]) and the estimated glomerular filtration rate (eGFR). Time-averaged proteinuria was defined as the average of urine protein to creatinine ratio (UPCR), measured every 3 months during both the trial and observational phases of the study.
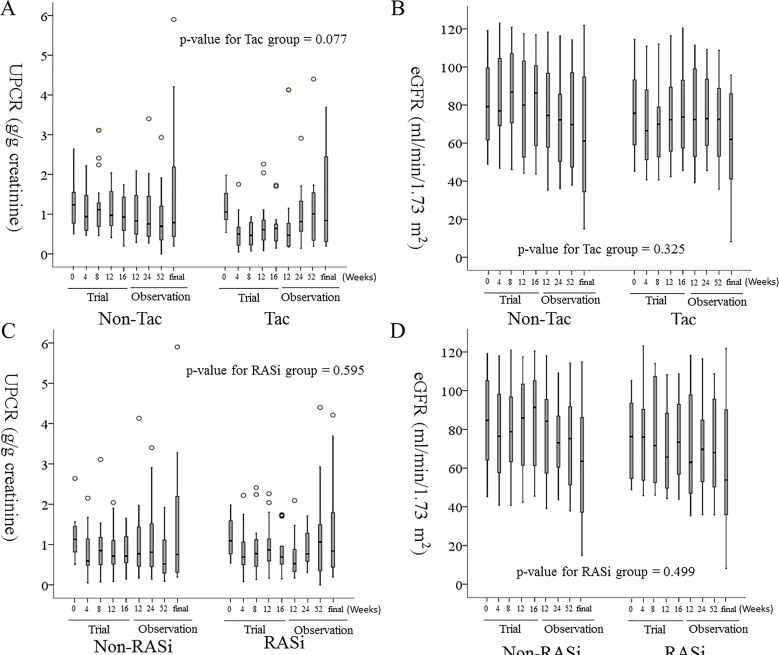
A significant reduction in UPCR was observed in the Tac group compared to non-Tac group at the 4 and 8 week visits during the trial phase (p = 0.023 and p = 0.003, respectively). However, the difference between the Tac group and non-Tac group was not evident in the other review periods, estimated by linear mixed effect model. The percentage change in TA-proteinuria was greater in the Tac group than that in the corresponding control group (116 ± 96% vs. 63 ± 239%, p = 0.004). Therefore, during the observational phase, TA-proteinuria was not significantly different between the Tac group and the non-Tac group (1.150 ± 0.733 g/g cr vs. 1.455 ± 2.017 g/g cr, p = 0.775). The levels of eGFR throughout the observational phase were not significantly different between the two groups. Furthermore, the mean rate of eGFR change throughout both phases of the study was -6.4 ± 5.9 mL/min/1.73 m2/year in the non-Tac group and -5.4 ± 7.9 mL/min/1.73 m2/year in the Tac group (p = 0.988).
The anti-proteinuric effect of tacrolimus was promptly reversed 3 months after discontinuing the drug. The use of tacrolimus for a short period of time for patients with IgAN temporarily reduces proteinuria, but the data showed no long-term efficacy regarding proteinuria reduction and improvement of renal function.
免疫抑制药物他克莫司对免疫球蛋白A肾病(IgAN)患者具有降低蛋白尿的短期作用。我们的研究调查了停用他克莫司后对蛋白尿和肾功能的影响。
经活检证实为IgAN的患者纳入本研究,并随机分为两个治疗组。每个治疗组都有相应的对照组。第一组包括接受他克莫司治疗的患者(他克莫司组与非他克莫司组),第二组包括接受肾素血管紧张素系统阻滞剂治疗的患者(RASi组与非RASi组)。他克莫司组接受治疗长达16周,在最后一次就诊时停止使用他克莫司(试验阶段)。我们在第12、24、52和240周对患者进行跟踪(观察阶段)。检查的主要结局是时间平均蛋白尿(TA-蛋白尿;克/克肌酐[cr])和估计肾小球滤过率(eGFR)从试验阶段到观察阶段的百分比变化。时间平均蛋白尿定义为在研究的试验阶段和观察阶段每3个月测量一次的尿蛋白与肌酐比值(UPCR)的平均值。
在试验阶段的第4周和第8周就诊时,与非他克莫司组相比,他克莫司组的UPCR显著降低(分别为p = 0.023和p = 0.003)。然而,通过线性混合效应模型估计,在其他复查期,他克莫司组与非他克莫司组之间的差异不明显。他克莫司组TA-蛋白尿的百分比变化大于相应对照组(116±96%对63±239%,p = 0.004)。因此,在观察阶段,他克莫司组与非他克莫司组之间的TA-蛋白尿无显著差异(1.150±0.733克/克cr对1.455±2.017克/克cr,p = 0.775)。在整个观察阶段,两组的eGFR水平无显著差异。此外,在研究的两个阶段中,非他克莫司组的eGFR平均变化率为-6.4±5.9毫升/分钟/1.73平方米/年,他克莫司组为-5.4±7.9毫升/分钟/1.73平方米/年(p = 0.988)。
停用他克莫司3个月后,其抗蛋白尿作用迅速逆转。IgAN患者短期使用他克莫司可暂时降低蛋白尿,但数据显示在降低蛋白尿和改善肾功能方面无长期疗效。