Broyles Michael R
Department of Clinical Pharmacy and Laboratory Services, Five Rivers Medical Center, Pocahontas, Arkansas.
Open Forum Infect Dis. 2017 Oct 3;4(4):ofx213. doi: 10.1093/ofid/ofx213. eCollection 2017 Fall.
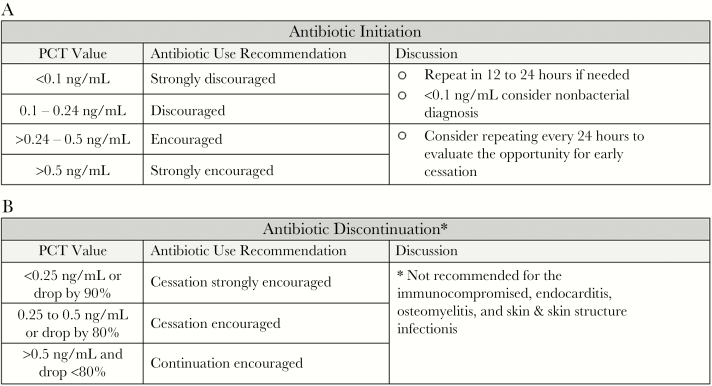
Delayed pathogen identification and nonspecific clinical findings make definitive decisions regarding antibiotics challenging. The stimuli of bacterial toxins and inflammation make procalcitonin (PCT) unique in its ability to differentiate bacterial infection from other causes of inflammation, and thus it is useful for antibiotic management. The objective of our study was to evaluate the impact of a PCT algorithm (PCT-A) on current practice.
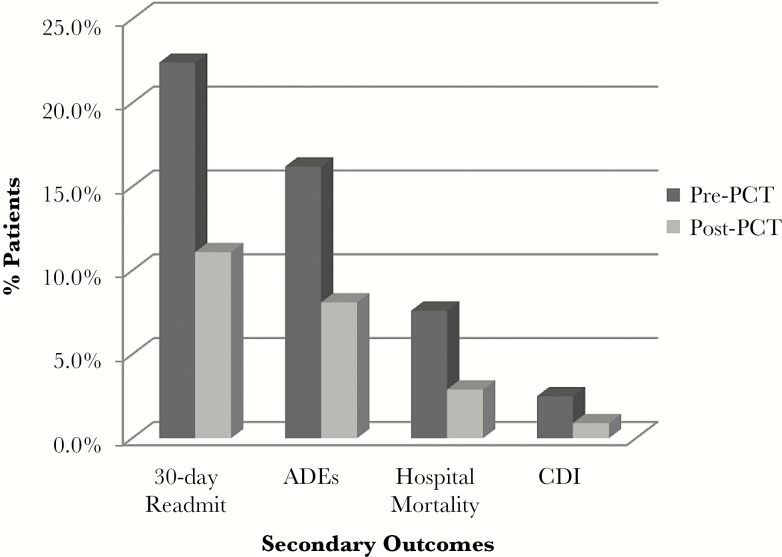
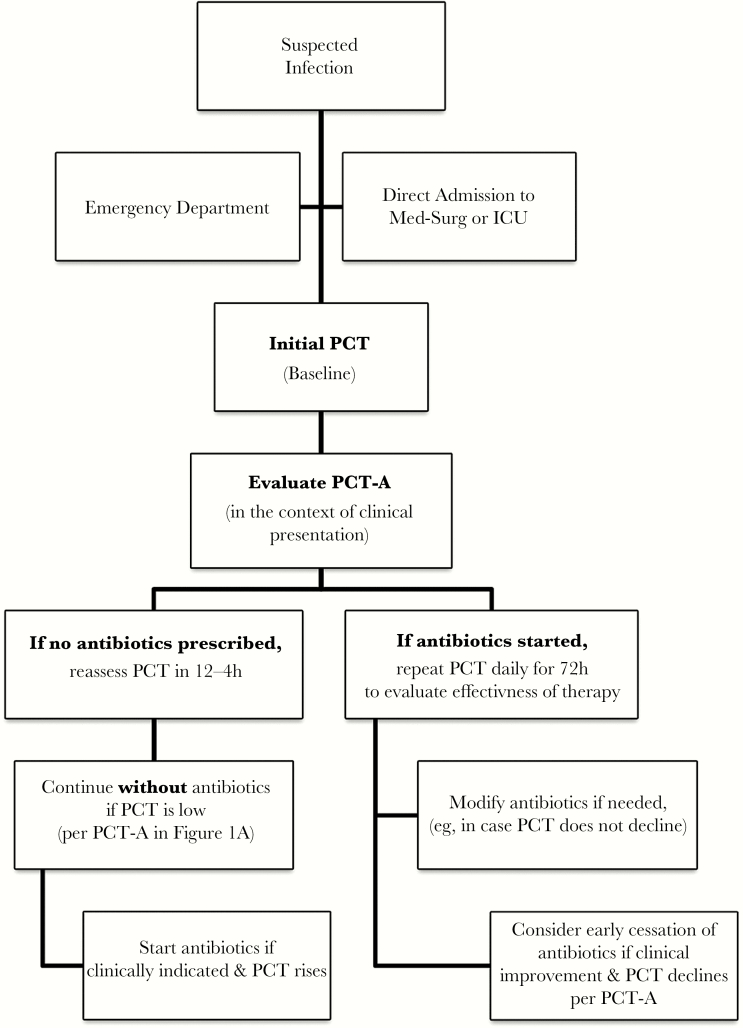
A single-center, retrospective cohort study was conducted to evaluate the impact of adding PCT-A to stewardship practices. Data from 4 years prior to and after PCT-A implementation were compared in critical and acute care patients of all ages receiving parenteral antibiotics for a DRG coded for infection. A baseline PCT was obtained on admission in patients with suspected bacterial infection. Serial PCT measurements were repeated daily to evaluate effectiveness of therapy. Outcomes of interest were antibiotic exposure, hospital mortality, 30-day readmission, infection (CDI), and adverse drug events during hospitalization.
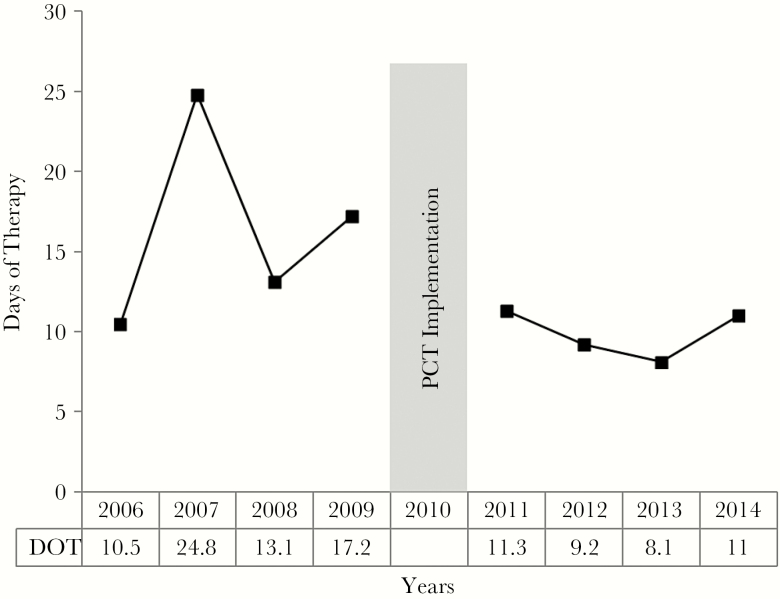
A total of 985 patients (pre-PCT-A group) were compared with 1167 patients (post-PCT-A group). Antimicrobial stewardship alone (pre-PCT-A) resulted in a median days of therapy (DOT) of 17 (interquartile range [IQR], 8.5-22.5) vs 9.0 (IQR, 6.5-12) in the post-PCT-A group ( < .0001). Secondary outcomes were also significantly reduced in the post-PCT-A group.
The addition of PCT in a facility with an established stewardship program resulted in a significant reduction in antibiotic exposure and adverse outcomes. PCT may improve antibiotic management when diagnostic clarity and resolution of infection are lacking.
病原菌鉴定延迟和非特异性临床症状使得在抗生素使用方面做出明确决策具有挑战性。细菌毒素和炎症刺激使得降钙素原(PCT)在区分细菌感染与其他炎症原因方面具有独特能力,因此它在抗生素管理中很有用。我们研究的目的是评估PCT算法(PCT-A)对当前实践的影响。
开展了一项单中心回顾性队列研究,以评估将PCT-A添加到管理措施中的影响。对实施PCT-A前后4年的数据进行比较,这些数据来自所有年龄接受肠外抗生素治疗且诊断相关分组(DRG)编码为感染的重症和急性护理患者。对疑似细菌感染患者入院时进行基线PCT检测。每天重复进行PCT系列检测以评估治疗效果。感兴趣的结果包括抗生素暴露、医院死亡率、30天再入院率、艰难梭菌感染(CDI)以及住院期间的药物不良事件。
共985例患者(PCT-A前组)与1167例患者(PCT-A后组)进行了比较。仅抗菌药物管理(PCT-A前)导致中位治疗天数(DOT)为17天(四分位间距[IQR],8.5 - 22.5),而PCT-A后组为9.0天(IQR,6.5 - 12)(P <.0001)。PCT-A后组的次要结果也显著降低。
在已建立管理项目的机构中添加PCT可显著减少抗生素暴露和不良后果。当缺乏感染诊断清晰度和感染解决方法时,PCT可能改善抗生素管理。