Valenzuela Espinoza Alexis, Devos Stefanie, van Hooff Robbert-Jan, Fobelets Maaike, Dupont Alain, Moens Maarten, Hubloue Ives, Lauwaert Door, Cornu Pieter, Brouns Raf, Putman Koen
Interuniversity Center for Health Economics Research, Vrije Universiteit Brussel, Brussels, Belgium.
Faculty of Medicine and Pharmacy, Vrije Universiteit Brussel, Brussels, Belgium.
JMIR Mhealth Uhealth. 2017 Nov 24;5(11):e175. doi: 10.2196/mhealth.8288.
Stroke is a very time-sensitive pathology, and many new solutions target the optimization of prehospital stroke care to improve the stroke management process. In-ambulance telemedicine, defined by live bidirectional audio-video between a patient and a neurologist in a moving ambulance and the automated transfer of vital parameters, is a promising new approach to speed up and improve the quality of acute stroke care. Currently, no evidence exists on the cost effectiveness of in-ambulance telemedicine.
We aim to develop a first cost effectiveness model for in-ambulance telemedicine and use this model to estimate the time savings needed before in-ambulance telemedicine becomes cost effective.
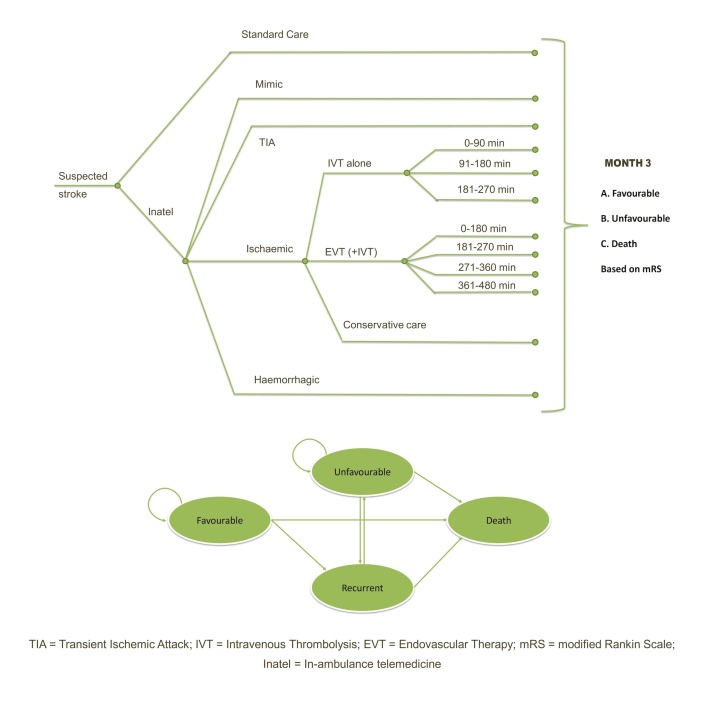
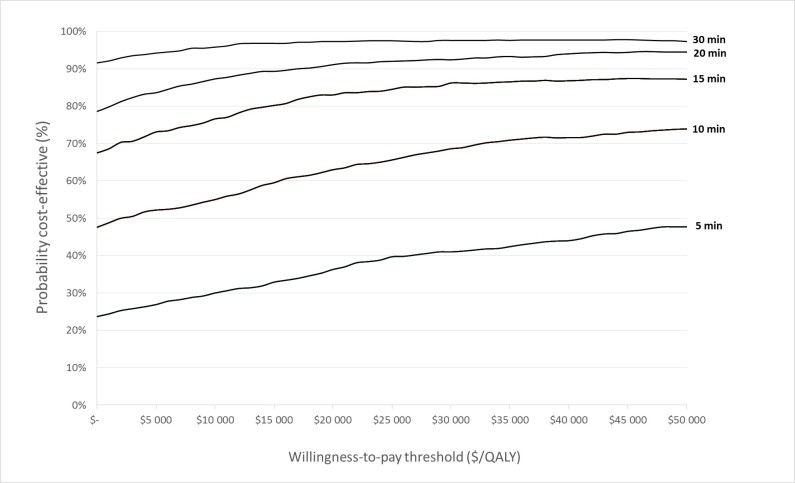
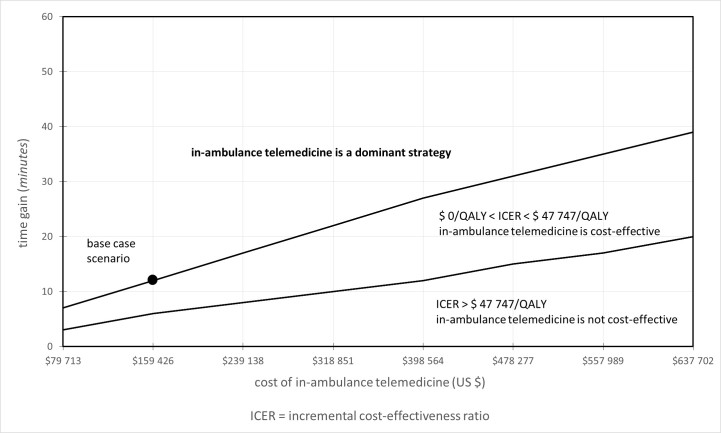
Current standard stroke care is compared with current standard stroke care supplemented with in-ambulance telemedicine using a cost-utility model measuring costs and quality-adjusted life-years (QALYs) from a health care perspective. We combine a decision tree with a Markov model. Data from the UZ Brussel Stroke Registry (2282 stroke patients) and linked hospital claims data at individual level are combined with literature data to populate the model. A 2-way sensitivity analysis varying both implementation costs and time gain is performed to map the different cost-effective combinations and identify the time gain needed for cost effectiveness and dominance. For several modeled time gains, the cost-effectiveness acceptability curve is calculated and mapped in 1 figure.
Under the base-case scenario (implementation cost of US $159,425) and taking a lifetime horizon into account, in-ambulance telemedicine is a cost-effective strategy compared to standard stroke care alone starting from a time gain of 6 minutes. After 12 minutes, in-ambulance telemedicine becomes dominant, and this results in a mean decrease of costs by US -$30 (95% CI -$32 to -$29) per patient with 0.00456 (95% CI 0.00448 to 0.00463) QALYs on average gained per patient. In over 82% of all probabilistic simulations, in-ambulance telemedicine remains under the cost-effectiveness threshold of US $47,747.
Our model suggests that in-ambulance telemedicine can be cost effective starting from a time gain of 6 minutes and becomes a dominant strategy after approximately 15 minutes. This indicates that in-ambulance telemedicine has the potential to become a cost-effective intervention assuming time gains in clinical implementations are realized in the future.
中风是一种对时间极为敏感的病症,许多新的解决方案旨在优化院前中风护理,以改善中风管理流程。救护车远程医疗是指在移动的救护车上患者与神经科医生之间进行实时双向音频 - 视频交流以及生命体征参数的自动传输,这是一种有望加快并提高急性中风护理质量的新方法。目前,尚无关于救护车远程医疗成本效益的证据。
我们旨在开发首个救护车远程医疗成本效益模型,并使用该模型估算在救护车远程医疗变得具有成本效益之前所需节省的时间。
使用从医疗保健角度衡量成本和质量调整生命年(QALYs)的成本效用模型,将当前标准中风护理与补充了救护车远程医疗的当前标准中风护理进行比较。我们将决策树与马尔可夫模型相结合。来自UZ布鲁塞尔中风登记处(2282名中风患者)的数据以及个体层面的关联医院理赔数据与文献数据相结合,以填充模型。进行双向敏感性分析,同时改变实施成本和时间增益,以绘制不同的成本效益组合,并确定成本效益和优势所需的时间增益。对于几个模拟的时间增益,计算成本效益可接受性曲线并绘制在一张图中。
在基准情景(实施成本为159,425美元)下,并考虑终身视角,与仅采用标准中风护理相比,从节省6分钟时间开始,救护车远程医疗就是一种具有成本效益的策略。12分钟后,救护车远程医疗变得占优,这导致每位患者平均成本降低30美元(95%CI -32美元至 -29美元),每位患者平均获得0.00456(95%CI 0.00448至0.00463)个QALYs。在超过82%的概率模拟中,救护车远程医疗仍低于47,747美元的成本效益阈值。
我们的模型表明,从节省6分钟时间开始,救护车远程医疗可能具有成本效益,大约15分钟后成为占优策略。这表明,如果未来在临床实施中实现时间增益,救护车远程医疗有可能成为一种具有成本效益的干预措施。