Berger Miles, Ponnusamy Vikram, Greene Nathaniel, Cooter Mary, Nadler Jacob W, Friedman Allan, McDonagh David L, Laskowitz Daniel T, Newman Mark F, Shaw Leslie M, Warner David S, Mathew Joseph P, James Michael L
Department of Anesthesiology, Duke University Medical Center, Durham, NC, United States.
University of Missouri School of Medicine, Columbia, MO, United States.
Front Immunol. 2017 Nov 13;8:1528. doi: 10.3389/fimmu.2017.01528. eCollection 2017.
Aside from direct effects on neurotransmission, inhaled and intravenous anesthetics have immunomodulatory properties. and mouse model studies suggest that propofol inhibits, while isoflurane increases, neuroinflammation. If these findings translate to humans, they could be clinically important since neuroinflammation has detrimental effects on neurocognitive function in numerous disease states.
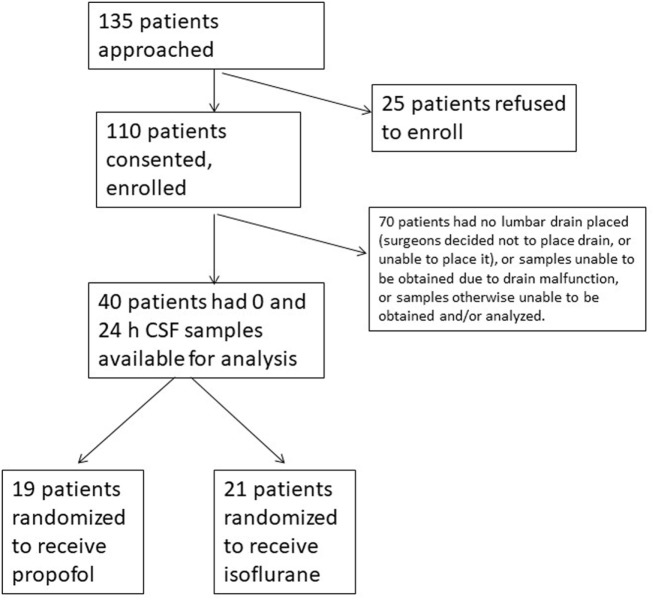
To examine whether propofol and isoflurane differentially modulate neuroinflammation in humans, cytokines were measured in a secondary analysis of cerebrospinal fluid (CSF) samples from patients prospectively randomized to receive anesthetic maintenance with propofol vs. isoflurane (registered with http://www.clinicaltrials.gov, identifier NCT01640275). We measured CSF levels of EGF, eotaxin, G-CSF, GM-CSF, IFN-α2, IL-1RA, IL-6, IL-7, IL-8, IL-10, IP-10, MCP-1, MIP-1α, MIP-1β, and TNF-α before and 24 h after intracranial surgery in these study patients.
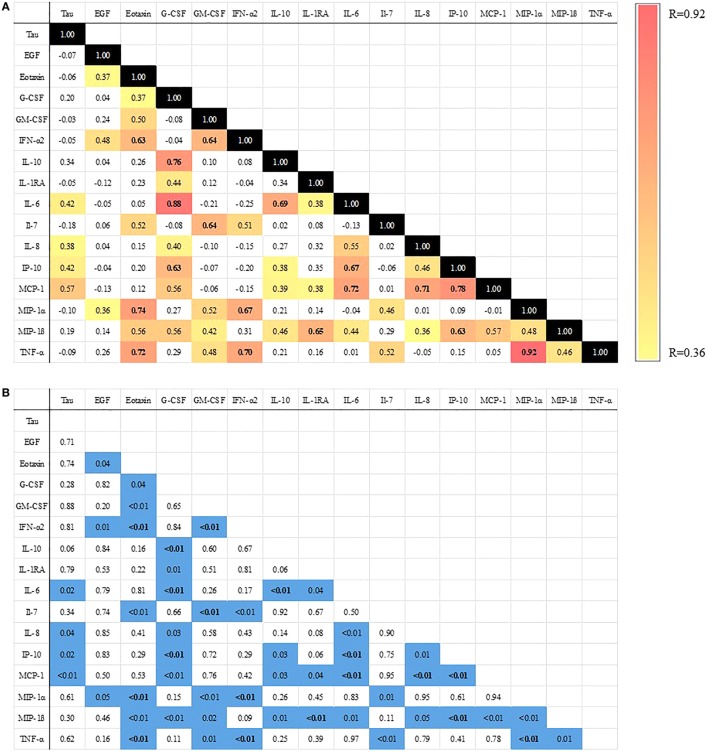
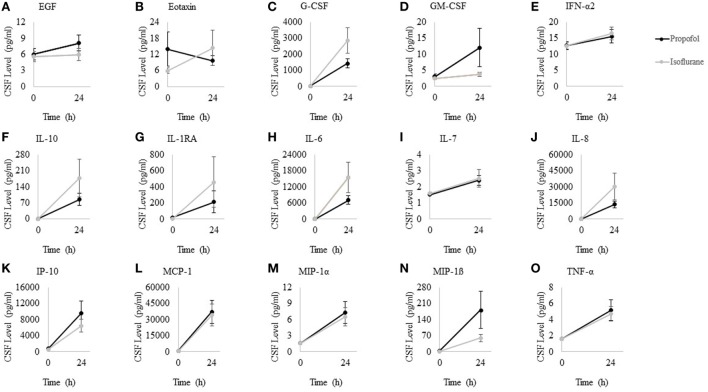
After Bonferroni correction for multiple comparisons, we found significant increases from before to 24 h after surgery in G-CSF, IL-10, IL-1RA, IL-6, IL-8, IP-10, MCP-1, MIP-1α, MIP-1β, and TNF-α. However, we found no difference in cytokine levels at baseline or 24 h after surgery between propofol- ( = 19) and isoflurane-treated ( = 21) patients ( > 0.05 for all comparisons). Increases in CSF IL-6, IL-8, IP-10, and MCP-1 levels directly correlated with each other and with postoperative CSF elevations in tau, a neural injury biomarker. We observed CSF cytokine increases up to 10-fold higher after intracranial surgery than previously reported after other types of surgery.
These data clarify the magnitude of neuroinflammation after intracranial surgery, and raise the possibility that a coordinated neuroinflammatory response may play a role in neural injury after surgery.
除了对神经传递的直接影响外,吸入性和静脉麻醉药还具有免疫调节特性。小鼠模型研究表明,丙泊酚具有抑制作用,而异氟烷会增加神经炎症。如果这些发现适用于人类,那么它们可能具有临床重要性,因为神经炎症在多种疾病状态下都会对神经认知功能产生不利影响。
为了研究丙泊酚和异氟烷是否对人类神经炎症有不同的调节作用,我们对前瞻性随机接受丙泊酚或异氟烷麻醉维持的患者脑脊液(CSF)样本进行了二次分析,以测量细胞因子水平(该研究已在http://www.clinicaltrials.gov注册,标识符为NCT01640275)。我们测量了这些研究患者颅内手术前和术后24小时脑脊液中表皮生长因子(EGF)、嗜酸性粒细胞趋化因子、粒细胞集落刺激因子(G-CSF)、粒细胞-巨噬细胞集落刺激因子(GM-CSF)、干扰素-α2、白细胞介素-1受体拮抗剂(IL-1RA)、白细胞介素-6(IL-6)、白细胞介素-7(IL-7)、白细胞介素-8(IL-8)、白细胞介素-10(IL-10)、干扰素诱导蛋白10(IP-10)、单核细胞趋化蛋白-1(MCP-1)、巨噬细胞炎性蛋白-1α(MIP-1α)、巨噬细胞炎性蛋白-1β(MIP-1β)和肿瘤坏死因子-α(TNF-α)的水平。
在进行多重比较的Bonferroni校正后,我们发现术后24小时与术前相比,G-CSF、IL-10、IL-1RA、IL-6、IL-8、IP-10、MCP-1、MIP-1α、MIP-1β和TNF-α有显著升高。然而,我们发现丙泊酚治疗组(n = 19)和异氟烷治疗组(n = 21)患者在基线或术后24小时的细胞因子水平没有差异(所有比较P>0.05)。脑脊液中IL-6、IL-8、IP-10和MCP-1水平的升高彼此直接相关,并且与神经损伤生物标志物tau蛋白术后脑脊液升高相关。我们观察到颅内手术后脑脊液细胞因子升高幅度比之前报道的其他类型手术高10倍。
这些数据阐明了颅内手术后神经炎症的程度,并提出了协同神经炎症反应可能在术后神经损伤中起作用的可能性。