Huang Yao-Kuang, Yen Chieh-Ling, Shiu Sz-Iuan, Lee Shou-Wu, Chang Pi-Yi, Yeh Hong-Zen, Lee Teng-Yu
Division of Gastroenterology & Hepatology, Department of Internal Medicine, Taichung Veterans General Hospital, Taichung, Taiwan.
Department of Medicine, Chung Shan Medical University, Taichung, Taiwan.
PLoS One. 2017 Nov 30;12(11):e0188999. doi: 10.1371/journal.pone.0188999. eCollection 2017.
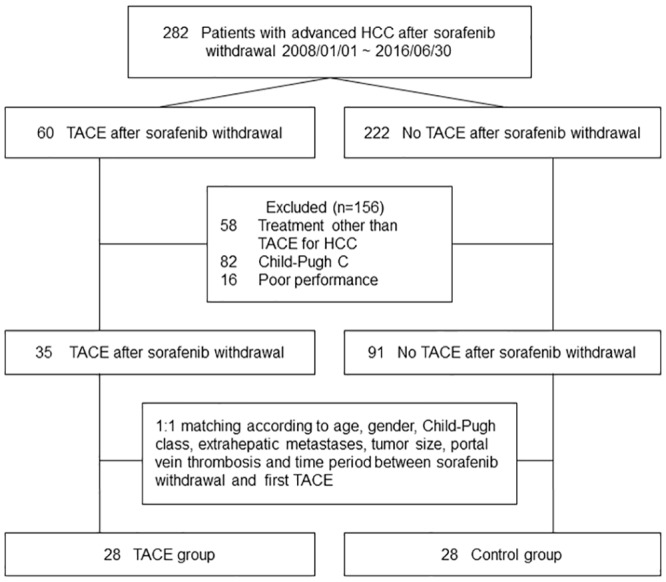
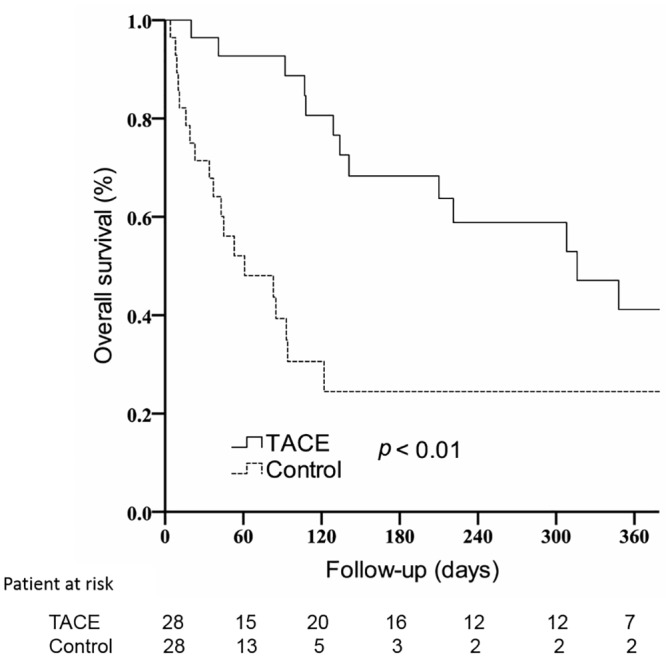
Targeted therapy is currently the standard treatment for advanced hepatocellular carcinoma (HCC), but an effective treatment after the discontinuation of sorafenib therapy remains uncertain. We aim to investigate the survival benefits of transcatheter arterial chemoembolization (TACE) after stopping sorafenib therapy. We retrospectively analyzed all patients with advanced HCC, who had received palliative TACE after terminating sorafenib therapy, from January 2008 to June 2016. Patients who were in the terminal stage (Child-Pugh class C or performance status 3-4), who received a liver transplantation, or who had received any HCC treatment other than TACE, were excluded. Finally, 28 patients were recruited as the TACE group, and were randomly matched 1:1 by age, gender, Child-Pugh class, extrahepatic metastasis, and portal vein thrombosis with 28 controls who only received supportive care. For avoiding any immortal time bias, the index date of outcome follow-up was also matched. Cumulative incidences of, and hazard ratios (HRs) for, patient mortality were analyzed. The baseline demographic data between the TACE group and the control group were similar, but the 1-year overall survival rate in the TACE group was significantly higher than that of the control group (41.2%, 95% confidence interval [CI]: 19.4-63.0% vs. 24.5%, 95% CI: 6.3-42.7%; p < 0.01). In multivariate analysis, after adjusting for alpha-fetoprotein > 400ng/mL, Child-Pugh class B, and tumor extension > 50% of liver volume, TACE was independently associated with a decreased mortality risk(HR 0.19, 95% CI: 0.08-0.42). In addition, tumor extension > 50% of the liver was another independent prognostic factor associated with an increased mortality risk (HR 2.99, 95% CI: 1.31-6.82). Multivariate stratified analyses verified the association of TACE with a decreased mortality rate in each patient subgroup (all HR < 1.0). By controlling intrahepatic tumor growth, TACE may be a treatment option for use in improving patient survival in advanced HCC, after the termination of sorafenib therapy.
靶向治疗目前是晚期肝细胞癌(HCC)的标准治疗方法,但索拉非尼治疗中断后的有效治疗方法仍不明确。我们旨在研究停止索拉非尼治疗后经动脉化疗栓塞术(TACE)的生存获益。我们回顾性分析了2008年1月至2016年6月期间所有在终止索拉非尼治疗后接受姑息性TACE的晚期HCC患者。处于终末期(Child-Pugh C级或体能状态3 - 4级)、接受肝移植或接受过TACE以外的任何HCC治疗的患者被排除。最终,招募了28例患者作为TACE组,并按年龄、性别、Child-Pugh分级、肝外转移和门静脉血栓形成情况与28例仅接受支持治疗的对照组进行1:1随机匹配。为避免任何不朽时间偏倚,结局随访的索引日期也进行了匹配。分析了患者死亡率的累积发生率和风险比(HRs)。TACE组和对照组之间的基线人口统计学数据相似,但TACE组的1年总生存率显著高于对照组(41.2%,95%置信区间[CI]:19.4 - 63.0%对24.5%,95%CI:6.3 - 42.7%;p < 0.01)。在多变量分析中,在调整甲胎蛋白>400ng/mL、Child-Pugh B级和肿瘤范围>肝脏体积的50%后,TACE与死亡风险降低独立相关(HR 0.19,95%CI:0.08 - 0.42)。此外,肿瘤范围>肝脏的50%是另一个与死亡风险增加相关的独立预后因素(HR 2.99,95%CI:1.31 - 6.82)。多变量分层分析证实了TACE与每个患者亚组死亡率降低之间的关联(所有HR < 1.0)。通过控制肝内肿瘤生长,TACE可能是索拉非尼治疗终止后用于改善晚期HCC患者生存的一种治疗选择。