Johns Hopkins Drug Discovery, Johns Hopkins School of Medicine, Baltimore, Maryland.
Medpace, Cincinnati, Ohio.
Cancer Res. 2018 Feb 1;78(3):817-829. doi: 10.1158/0008-5472.CAN-17-1467. Epub 2017 Nov 30.
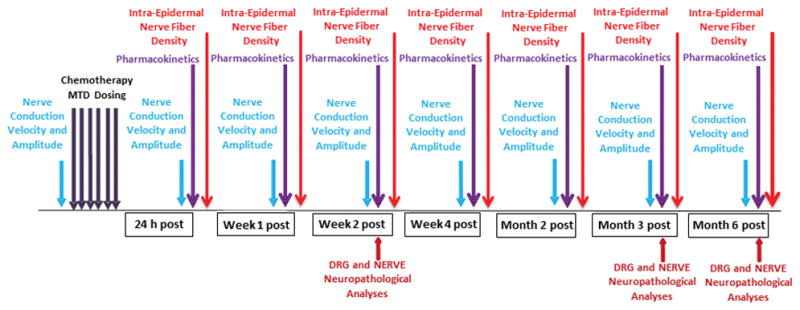
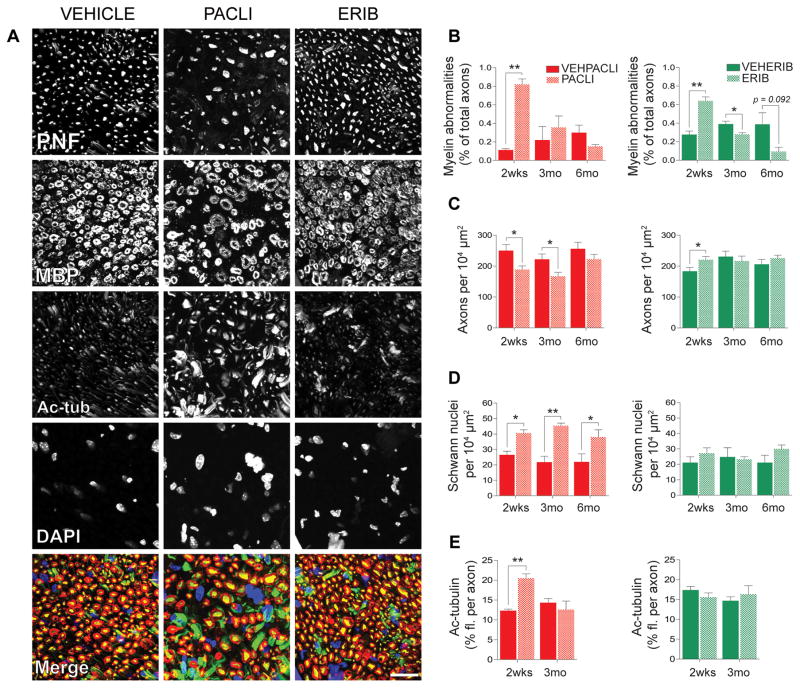
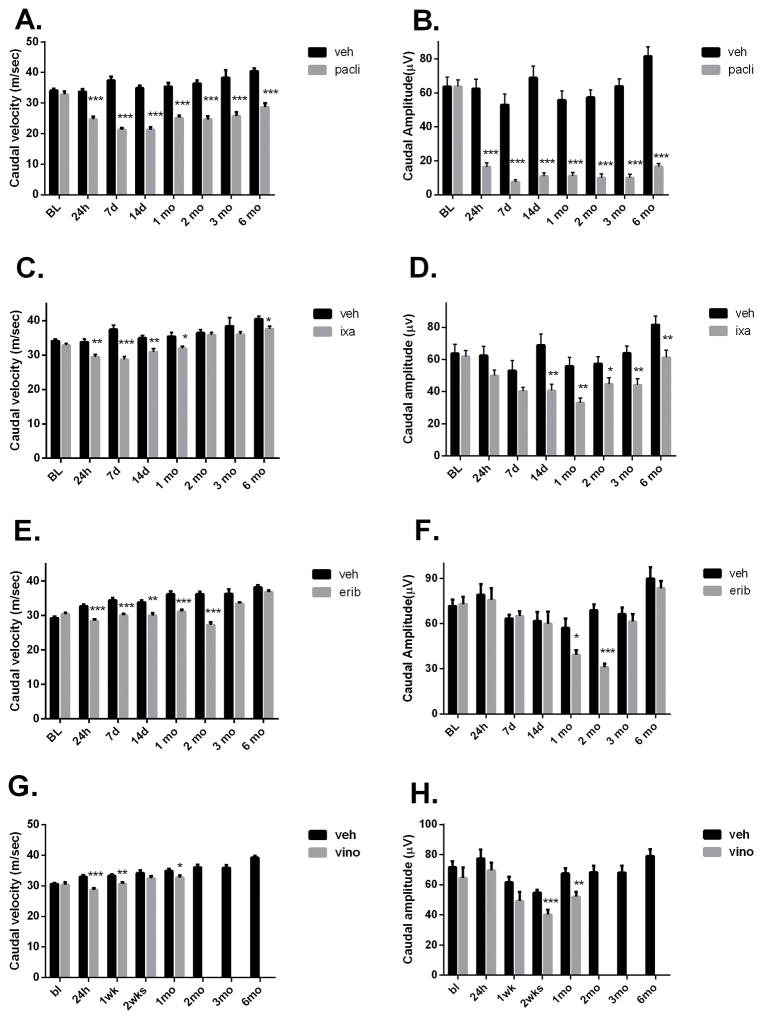
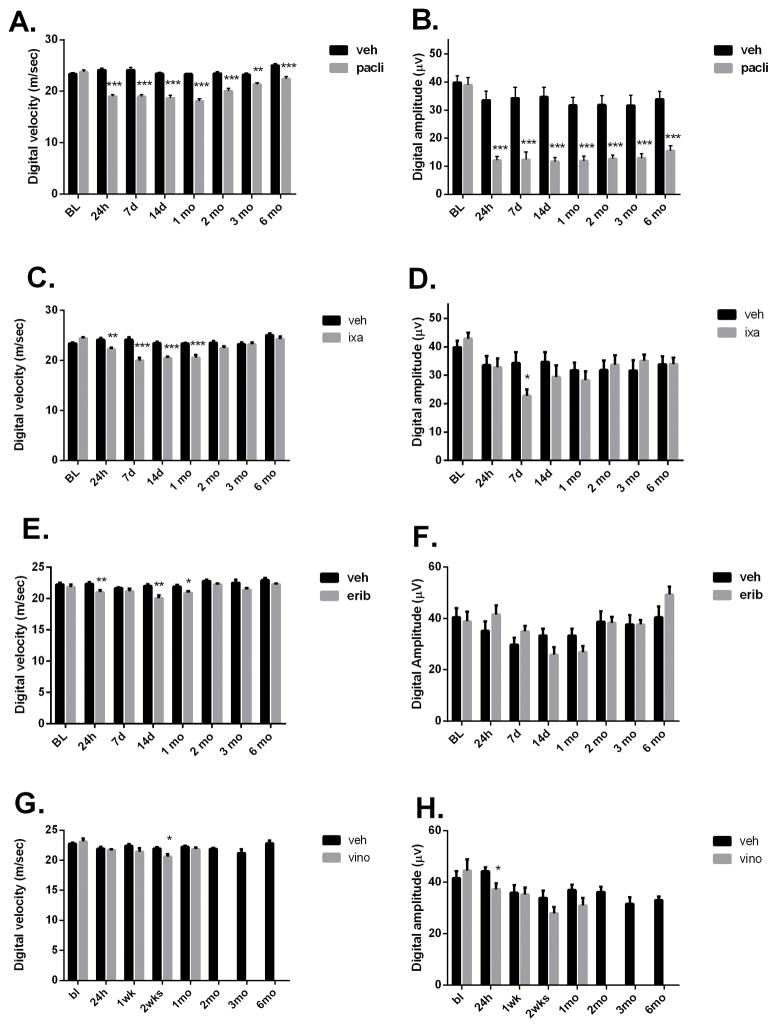
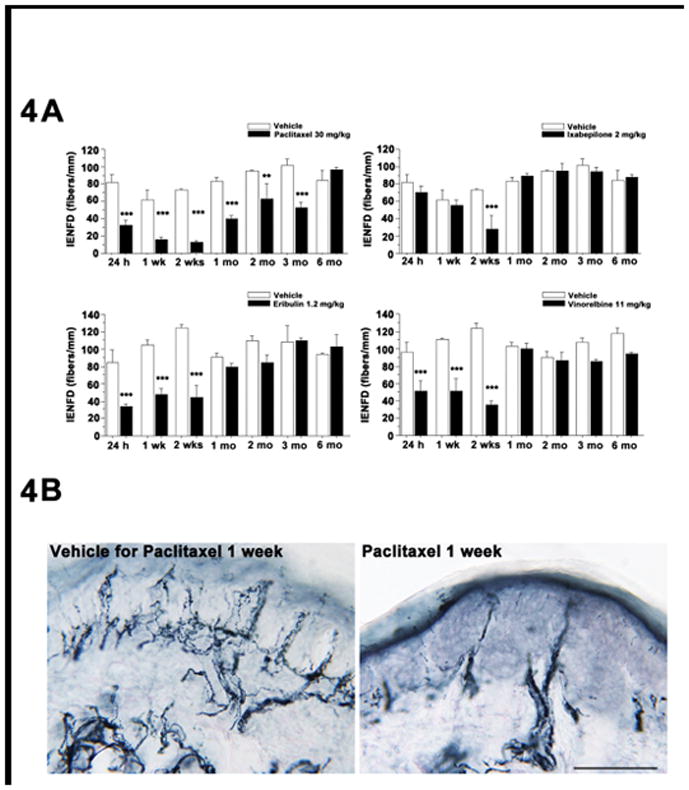
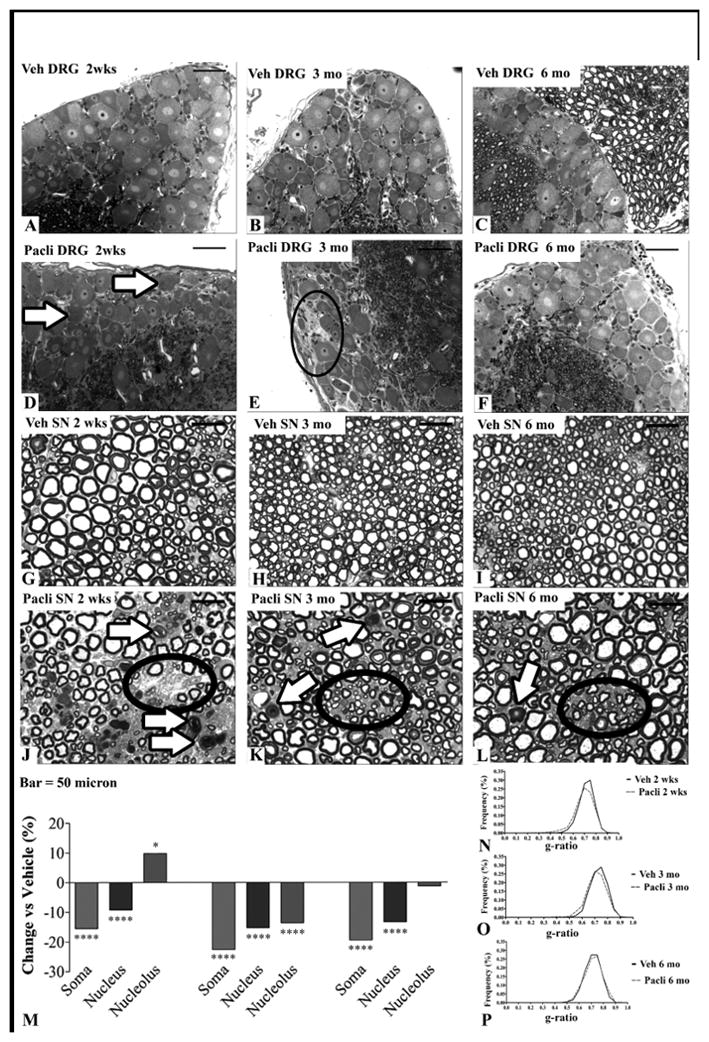
Chemotherapy-induced peripheral neuropathy (CIPN) is a major cause of disability in cancer survivors. CIPN investigations in preclinical model systems have focused on either behaviors or acute changes in nerve conduction velocity (NCV) and amplitude, but greater understanding of the underlying nature of axonal injury and its long-term processes is needed as cancer patients live longer. In this study, we used multiple independent endpoints to systematically characterize CIPN recovery in mice exposed to the antitubulin cancer drugs eribulin, ixabepilone, paclitaxel, or vinorelbine at MTDs. All of the drugs ablated intraepidermal nerve fibers and produced axonopathy, with a secondary disruption in myelin structure within 2 weeks of drug administration. In addition, all of the drugs reduced sensory NCV and amplitude, with greater deficits after paclitaxel and lesser deficits after ixabepilone. These effects correlated with degeneration in dorsal root ganglia (DRG) and sciatic nerve and abundance of Schwann cells. Although most injuries were fully reversible after 3-6 months after administration of eribulin, vinorelbine, and ixabepilone, we observed delayed recovery after paclitaxel that produced a more severe, pervasive, and prolonged neurotoxicity. Compared with other agents, paclitaxel also displayed a unique prolonged exposure in sciatic nerve and DRG. The most sensitive indicator of toxicity was axonopathy and secondary myelin changes accompanied by a reduction in intraepidermal nerve fiber density. Taken together, our findings suggest that intraepidermal nerve fiber density and changes in NCV and amplitude might provide measures of axonal injury to guide clinical practice. This detailed preclinical study of the long-term effects of widely used antitubulin cancer drugs on the peripheral nervous system may help guide clinical evaluations to improve personalized care in limiting neurotoxicity in cancer survivors. .
化疗引起的周围神经病(CIPN)是癌症幸存者残疾的主要原因。在临床前模型系统中,CIPN 的研究主要集中在行为或神经传导速度(NCV)和幅度的急性变化上,但需要更好地了解轴突损伤的潜在性质及其长期过程,因为癌症患者的寿命更长。在这项研究中,我们使用多个独立的终点来系统地描述在 MTD 下暴露于抗癌药物艾日布林、伊沙匹隆、紫杉醇或长春瑞滨的小鼠中的 CIPN 恢复情况。所有药物均消融了表皮内神经纤维并引起轴突病,在药物给药后 2 周内继发髓鞘结构中断。此外,所有药物均降低了感觉 NCV 和幅度,紫杉醇后降幅更大,伊沙匹隆后降幅更小。这些影响与背根神经节(DRG)和坐骨神经的变性以及雪旺细胞的丰度相关。尽管在艾日布林、长春瑞滨和伊沙匹隆给药后 3-6 个月后,大多数损伤完全可逆,但我们观察到紫杉醇引起的延迟恢复,导致更严重、更普遍和更持久的神经毒性。与其他药物相比,紫杉醇在坐骨神经和 DRG 中也表现出独特的延长暴露。毒性的最敏感指标是轴突病和继发髓鞘变化,伴有表皮内神经纤维密度降低。总之,我们的研究结果表明,表皮内神经纤维密度以及 NCV 和幅度的变化可能为指导临床实践提供轴突损伤的指标。这项对广泛使用的抗癌药物对周围神经系统的长期影响的详细临床前研究可能有助于指导临床评估,以改善对癌症幸存者神经毒性的个性化护理。