Lichtensztajn Daphne Y, Giddings Brenda M, Morris Cyllene R, Parikh-Patel Arti, Kizer Kenneth W
Greater Bay Area Cancer Registry, Cancer Prevention Institute of California, CA, USA.
California Cancer Reporting and Epidemiologic Surveillance Program, Institute for Population Health Improvement, UC Davis Health, CA, USA.
Clin Epidemiol. 2017 Nov 20;9:601-609. doi: 10.2147/CLEP.S146395. eCollection 2017.
The presence of comorbid medical conditions can significantly affect a cancer patient's treatment options, quality of life, and survival. However, these important data are often lacking from population-based cancer registries. Leveraging routine linkage to hospital discharge data, a comorbidity score was calculated for patients in the California Cancer Registry (CCR) database.
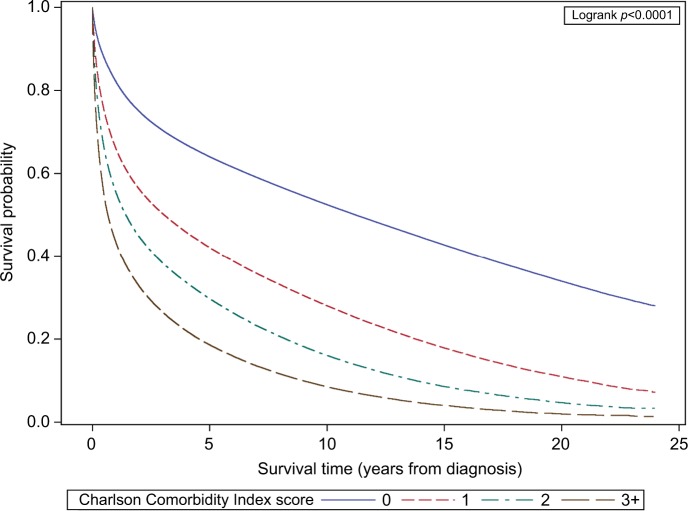
California cancer cases diagnosed between 1991 and 2013 were linked to statewide hospital discharge data. A Deyo and Romano adapted Charlson Comorbidity Index was calculated for each case, and the association of comorbidity score with overall survival was assessed with Kaplan-Meier curves and Cox proportional hazards models. Using a subset of Medicare-enrolled CCR cases, the index was validated against a comorbidity score derived using Surveillance, Epidemiology, and End Results (SEER)-Medicare linked data.
A comorbidity score was calculated for 71% of CCR cases. The majority (60.2%) had no relevant comorbidities. Increasing comorbidity score was associated with poorer overall survival. In a multivariable model, high comorbidity conferred twice the risk of death compared to no comorbidity (hazard ratio 2.33, 95% CI: 2.32-2.34). In the subset of patients with a SEER-Medicare-derived score, the sensitivity of the hospital discharge-based index for detecting any comorbidity was 76.5. The association between overall mortality and comorbidity score was stronger for the hospital discharge-based score than for the SEER-Medicare-derived index, and the predictive ability of the hospital discharge-based score, as measured by Harrell's C index, was also slightly better for the hospital discharge-based score (C index 0.62 versus 0.59, <0.001).
Despite some limitations, using hospital discharge data to construct a comorbidity index for cancer registries is a feasible and valid method to enhance registry data, which can provide important clinically relevant information for population-based cancer outcomes research.
合并症的存在会显著影响癌症患者的治疗选择、生活质量和生存率。然而,基于人群的癌症登记处往往缺乏这些重要数据。通过利用与医院出院数据的常规链接,为加利福尼亚癌症登记处(CCR)数据库中的患者计算了合并症评分。
将1991年至2013年期间诊断出的加利福尼亚癌症病例与全州医院出院数据进行链接。为每个病例计算了经过Deyo和Romano改编的Charlson合并症指数,并使用Kaplan-Meier曲线和Cox比例风险模型评估合并症评分与总生存率之间的关联。使用一部分加入医疗保险的CCR病例子集,将该指数与使用监测、流行病学和最终结果(SEER)-医疗保险链接数据得出的合并症评分进行验证。
为71%的CCR病例计算了合并症评分。大多数(60.2%)没有相关合并症。合并症评分增加与较差的总生存率相关。在多变量模型中,与无合并症相比,高合并症使死亡风险增加两倍(风险比2.33,95%置信区间:2.32 - 2.34)。在具有SEER-医疗保险得出的评分的患者子集中,基于医院出院的指数检测任何合并症的敏感性为76.5。基于医院出院的评分与总死亡率之间的关联比基于SEER-医疗保险得出的指数更强,并且基于医院出院的评分的预测能力(通过Harrell's C指数衡量)也略优于基于SEER-医疗保险得出的指数(C指数0.62对0.59,<0.001)。
尽管存在一些局限性,但利用医院出院数据为癌症登记处构建合并症指数是增强登记处数据的一种可行且有效的方法,可为基于人群的癌症结局研究提供重要的临床相关信息。