Heo Ju-Yeong, Lee Ji-Won, Kim Cheol-Hwan, Lee Sang-Min, Choi Yong-Soo
Department of Orthopedic Surgery, Kwangju Christian Hospital, Gwangju, Korea.
Clin Orthop Surg. 2017 Dec;9(4):472-479. doi: 10.4055/cios.2017.9.4.472. Epub 2017 Nov 10.
The role of ultrasound in the thoracic spine has been underappreciated, partly because of the relative efficacy of the landmark-guided technique and the limitation of imaging through the narrow acoustic windows produced by the bony framework of thoracic spine. The aim of this study was to make a comparison between the 12th rib and the spinous process of C7 as a landmark for effective ultrasound-guided target segment identification in the thoracic spine.
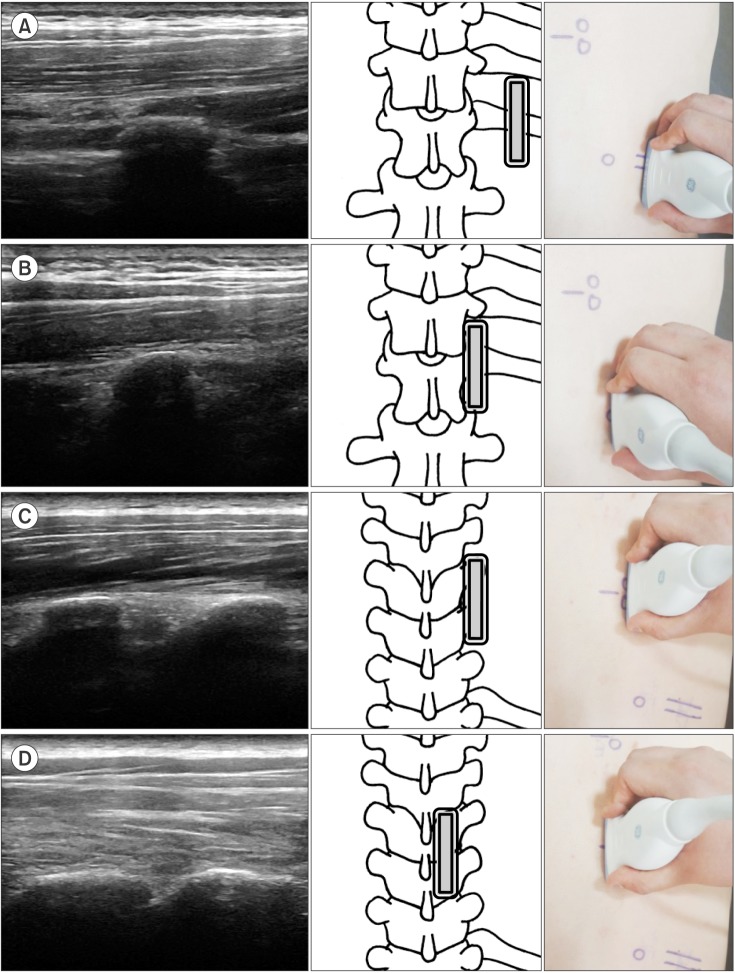
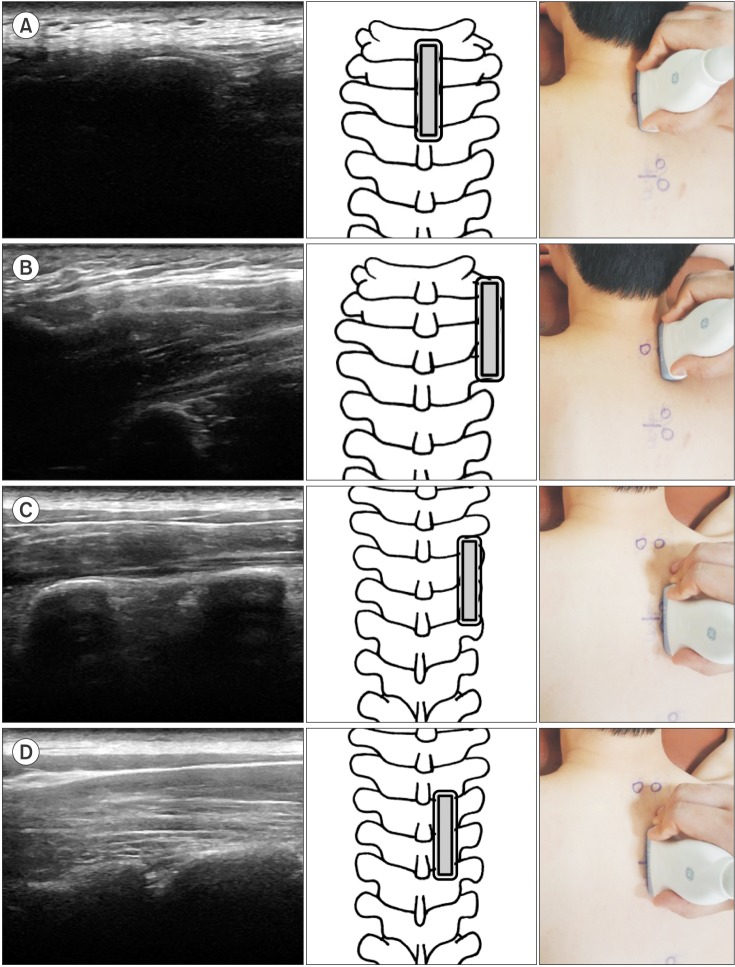
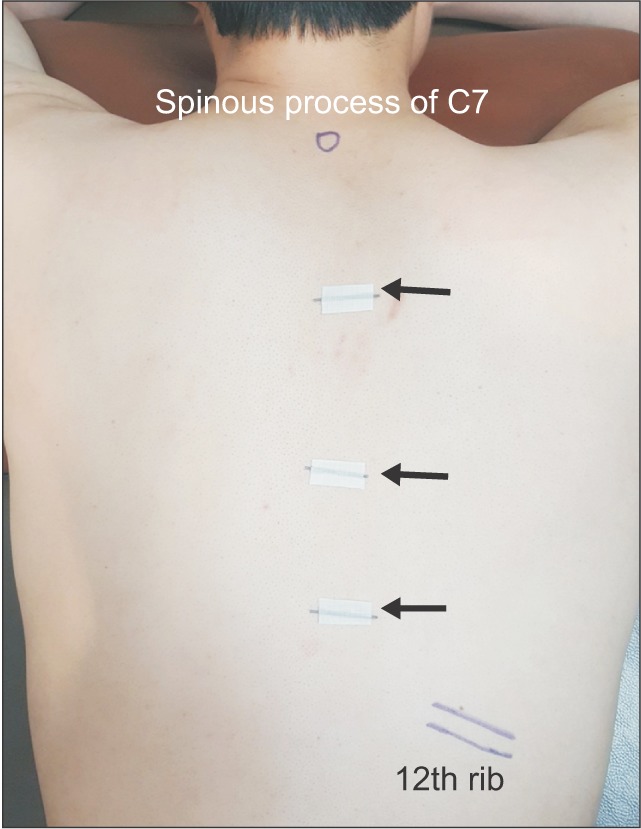
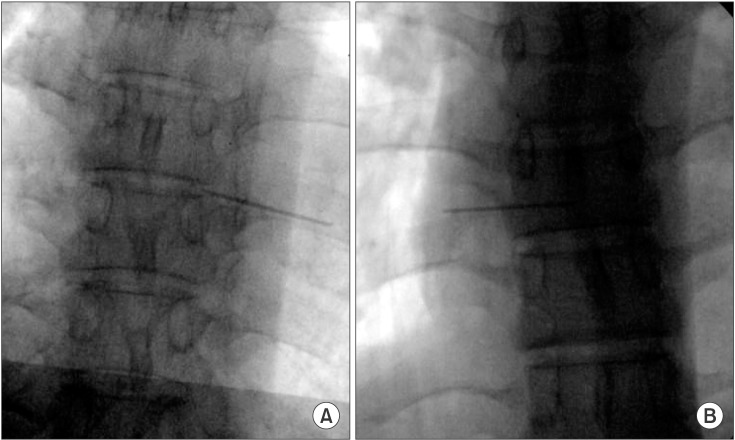
Ultrasonography of 44 thoracic spines was performed and the same procedure was carried out 1 week later again. The target segments (T3-4, T7-8, and T10-11) were identified using the 12th rib (group 1) or the spinous process of C7 (group 2) as a starting landmark. Ultrasound scanning was done proximally (group 1) or distally (group 2) toward the target transverse process and further medially and slightly superior to the target thoracic facet. Then, a metal marker was placed on the T3-4, T7-8, and T10-11 and the location of each marker was confirmed by fluoroscopy.
In the total 132 segments, sonographic identification was confirmed to be successful with fluoroscopy in 84.1% in group 1 and 56.8% in group 2. Group 1 had a greater success rate in ultrasound-guided target segment identification than group 2 ( = 0.001), especially in T10-11 (group 1, 93.2%; group 2, 43.2%; = 0.001) and T7-8 (group 1, 86.4%; group 2, 56.8%; = 0.002). The intrarater reliability of ultrasound-guided target segment identification was good (group 1, = 0.76; group 2, = 0.82), showing no difference between right and left sides. Ultrasound-guided target segment identification was more effective in the non-obese subjects ( = 0.001), especially in group 1.
Ultrasound-guided detection using the 12th rib as a starting landmark for scanning could be a promising technique for successful target segment identification in the thoracic spine.
超声在胸椎中的作用一直未得到充分重视,部分原因是体表标志引导技术的相对有效性以及通过胸椎骨框架产生的狭窄声窗进行成像的局限性。本研究的目的是比较第12肋和C7棘突作为超声引导下胸椎有效目标节段识别标志的效果。
对44个胸椎进行超声检查,并在1周后再次进行相同操作。使用第12肋(第1组)或C7棘突(第2组)作为起始标志来识别目标节段(T3 - 4、T7 - 8和T10 - 11)。向目标横突近端(第1组)或远端(第2组)进行超声扫描,并进一步向内侧且略高于目标胸椎小关节处扫描。然后,在T3 - 4、T7 - 8和T10 - 11处放置金属标记物,并通过荧光透视确认每个标记物的位置。
在总共132个节段中,第1组超声识别并经荧光透视确认成功的比例为84.1%,第2组为56.8%。第1组在超声引导下目标节段识别的成功率高于第2组(P = 0.001),尤其是在T10 - 11(第1组,93.2%;第2组,43.2%;P = 0.001)和T7 - 8(第1组,86.4%;第2组,56.8%;P = 0.002)。超声引导下目标节段识别的观察者内可靠性良好(第1组,κ = 0.76;第2组,κ = 0.82),左右两侧无差异。超声引导下目标节段识别在非肥胖受试者中更有效(P = 0.001),尤其是在第1组。
以第12肋作为起始标志进行超声引导检测可能是一种成功识别胸椎目标节段的有前景的技术。