Shady Waleed, Petre Elena N, Do Kinh Gian, Gonen Mithat, Yarmohammadi Hooman, Brown Karen T, Kemeny Nancy E, D'Angelica Michael, Kingham Peter T, Solomon Stephen B, Sofocleous Constantinos T
Section of Interventional Radiology, Department of Radiology, Memorial Sloan Kettering Cancer Center, 1275 York Avenue, New York, NY, 10065.
Department of Radiology, Memorial Sloan Kettering Cancer Center, 1275 York Avenue, New York, NY, 10065.
J Vasc Interv Radiol. 2018 Feb;29(2):268-275.e1. doi: 10.1016/j.jvir.2017.08.021. Epub 2017 Dec 6.
To identify and compare predictors of local tumor progression (LTP)-free survival (LTPFS) after radiofrequency (RF) ablation and microwave (MW) ablation of colorectal liver metastases (CLMs).
This is a retrospective review of CLMs ablated from November 2009 to April 2015 (110 patients). Margins were measured on contrast-enhanced computed tomography (CT) 6 weeks after ablation. Clinical and technical predictors of LTPFS were assessed using a competing risk model adjusted for clustering.
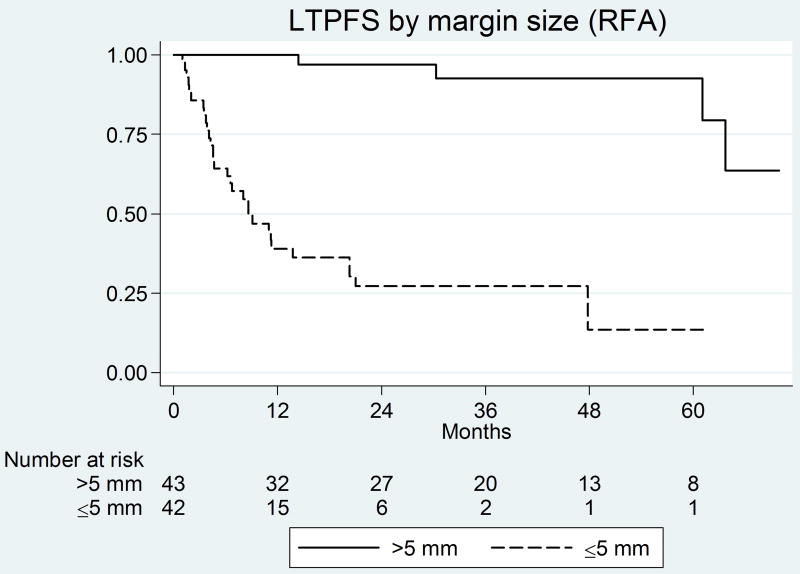
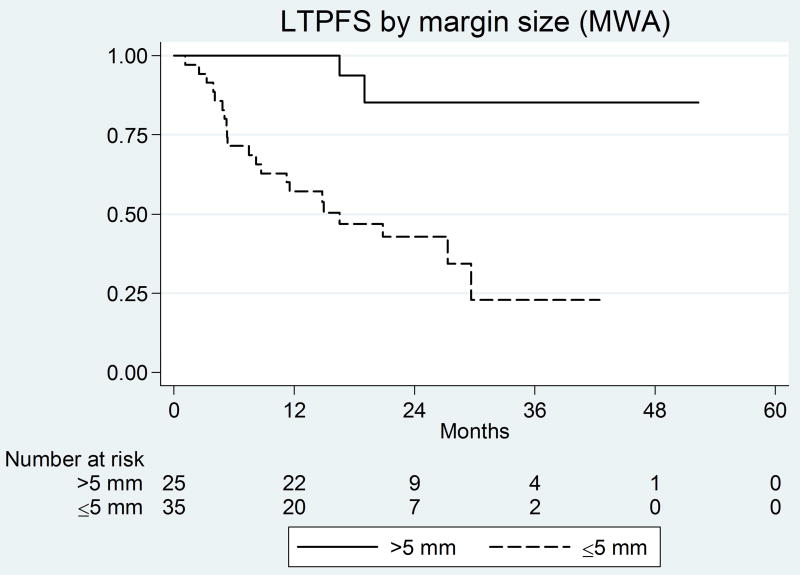
Technique effectiveness (complete ablation) was 93% (79/85) for RF ablation and 97% (58/60) for MW ablation (P = .47). The median follow-up period was significantly longer for RF ablation than for MW ablation (56 months vs. 29 months) (P < .001). There was no difference in the local tumor progression (LTP) rates between RF ablation and MW ablation (P = 0.84). Significant predictors of shorter LTPFS for RF ablation on univariate analysis were ablation margins 5 mm or smaller (P < .001) (hazard ratio [HR]: 14.6; 95% confidence interval [CI]: 5.2-40.9) and perivascular tumors (P = .021) (HR: 2.2; 95% CI: 1.1-4.3); both retained significance on multivariate analysis. Significant predictors of shorter LTPFS on univariate analysis for MW ablation were ablation margins 5 mm or smaller (P < .001) (subhazard ratio: 11.6; 95% CI: 3.1-42.7) and no history of prior liver resection (P < .013) (HR: 3.2; 95%: 1.3-7.8); both retained significance on multivariate analysis. There was no LTP for tumors ablated with margins over 10 mm (median LTPFS: not reached). Perivascular tumors were not predictive for MW ablation (P = .43).
Regardless of the thermal ablation modality used, margins larger than 5 mm are critical for local tumor control, with no LTP noted for margins over 10 mm. Unlike RF ablation, the efficiency of MW ablation was not affected for perivascular tumors.
识别并比较射频(RF)消融和微波(MW)消融结直肠癌肝转移瘤(CLM)后无局部肿瘤进展(LTP)生存期(LTPFS)的预测因素。
这是一项对2009年11月至2015年4月间接受消融治疗的CLM患者(110例)的回顾性研究。在消融后6周的对比增强计算机断层扫描(CT)上测量切缘。使用针对聚类进行调整的竞争风险模型评估LTPFS的临床和技术预测因素。
RF消融的技术有效性(完全消融)为93%(79/85),MW消融为97%(58/60)(P = 0.47)。RF消融的中位随访期显著长于MW消融(56个月对29个月)(P < 0.001)。RF消融和MW消融之间的局部肿瘤进展(LTP)率无差异(P = 0.84)。单因素分析中,RF消融LTPFS较短的显著预测因素为消融切缘5mm或更小(P < 0.001)(风险比[HR]:14.6;95%置信区间[CI]:5.2 - 40.9)和血管周围肿瘤(P = 0.021)(HR:2.2;95% CI:1.1 - 4.3);两者在多因素分析中仍具有显著性。MW消融单因素分析中LTPFS较短的显著预测因素为消融切缘5mm或更小(P < 0.001)(亚风险比:11.6;95% CI:3.1 - 42.7)和无既往肝切除史(P < 0.013)(HR:3.2;9�%:1.3 - 7.8);两者在多因素分析中仍具有显著性。切缘超过10mm消融的肿瘤未发生LTP(中位LTPFS:未达到)。血管周围肿瘤对MW消融无预测性(P = 0.43)。
无论采用何种热消融方式,大于5mm的切缘对局部肿瘤控制至关重要,切缘超过10mm未观察到LTP。与RF消融不同,MW消融的效率不受血管周围肿瘤的影响。