Tanuma Junko, Matsumoto Shoko, Haneuse Sebastien, Cuong Do Duy, Vu Tuong Van, Thuy Pham Thi Thanh, Dung Nguyen Thi, Dung Nguyen Thi Hoai, Trung Nguyen Vu, Kinh Nguyen Van, Oka Shinichi
AIDS Clinical Center, National Center for Global Health and Medicine, Tokyo, Japan.
Takemi Program in International Health, Harvard T.H. Chan School of Public Health, Boston, MA, USA.
J Int AIDS Soc. 2017 Dec;20(4). doi: 10.1002/jia2.25030.
Achieving viral suppression is key in the global strategy to end the HIV epidemic. However, the levels of viral suppression have yet to be described in many resource-limited settings.
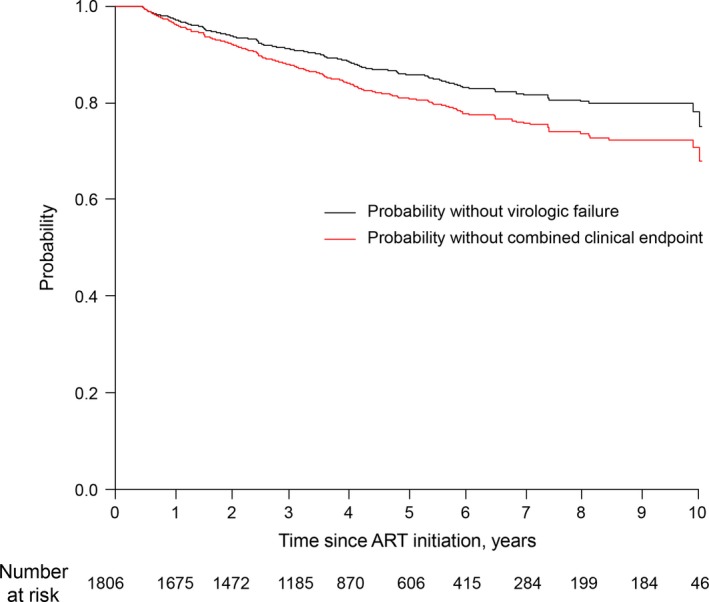
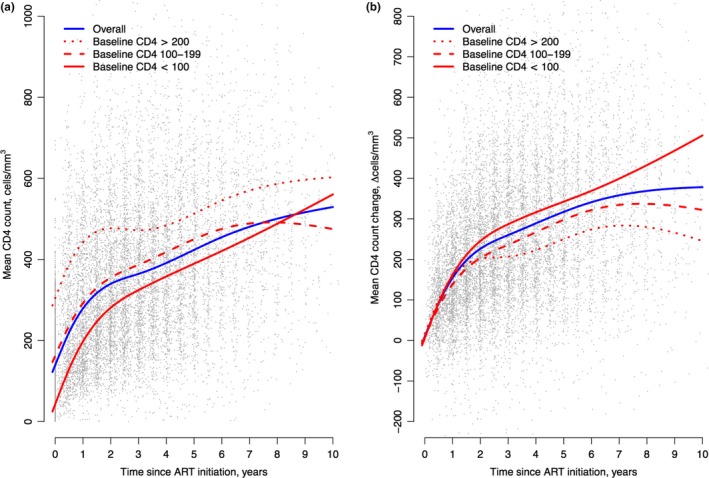
We investigated the time to virologic failure (VF; defined as a viral load of ≥1000 copies/ml) and changes in CD4 counts since starting antiretroviral therapy (ART) in a cohort of HIV-infected adults in Hanoi, Vietnam. Factors related to the time to VF and impaired early immune recovery (defined as not attaining an increase in 100 cells/mm in CD4 counts at 24 months) were further analysed.
From 1806 participants, 225 were identified as having VF at a median of 50 months of first-line ART. The viral suppression rate at 12 months was 95.5% and survival without VF was maintained above 90% until 42 months. An increase in CD4 counts from the baseline was greater in groups with lower baseline CD4 counts. A younger age (multivariate hazard ratio (HR) 0.75, vs. <30), hepatitis C (HCV)-antibody positivity (HR 1.43), and stavudine (d4T)-containing regimens (HR 1.4, vs. zidovudine (AZT)) were associated with earlier VF. Factors associated with impaired early immune recovery included the male sex (odds ratio (OR) 1.78), HCV-antibody positivity (OR 1.72), d4T-based regimens (OR 0.51, vs. AZT), and nevirapine-based regimens (OR 0.53, vs. efavirenz) after controlling for baseline CD4 counts.
Durable high-rate viral suppression was observed in the cohort of patients on first-line ART in Vietnam. Our results highlight the need to increase adherence support among injection drug users and HCV co-infected patients.
实现病毒抑制是全球终结艾滋病流行战略的关键。然而,在许多资源有限的环境中,病毒抑制水平尚未得到描述。
我们调查了越南河内一组感染艾滋病毒的成年人自开始抗逆转录病毒治疗(ART)以来的病毒学失败时间(VF;定义为病毒载量≥1000拷贝/毫升)以及CD4细胞计数的变化。进一步分析了与VF时间和早期免疫恢复受损(定义为在24个月时CD4细胞计数未增加100个细胞/立方毫米)相关的因素。
在1806名参与者中,225人在一线ART治疗的中位时间50个月时被确定为发生病毒学失败。12个月时的病毒抑制率为95.5%,在42个月之前无VF的生存率维持在90%以上。基线CD4细胞计数较低的组中,CD4细胞计数相对于基线的增加幅度更大。年龄较小(多变量风险比(HR)0.75,与<30岁相比)、丙型肝炎(HCV)抗体阳性(HR 1.43)以及含司他夫定(d4T)的治疗方案(HR 1.4,与齐多夫定(AZT)相比)与更早发生VF相关。在控制基线CD4细胞计数后,与早期免疫恢复受损相关的因素包括男性(优势比(OR)1.78)、HCV抗体阳性(OR 1.72)、基于d4T的治疗方案(OR 0.51,与AZT相比)以及基于奈韦拉平的治疗方案(OR 0.53,与依非韦伦相比)。
在越南接受一线ART治疗的患者队列中观察到了持久的高病毒抑制率。我们的结果强调了需要加强对注射吸毒者和HCV合并感染患者的依从性支持。