Cascio Rizzo Angelo, Paolucci Matteo, Altavilla Riccardo, Brunelli Nicoletta, Assenza Federica, Altamura Claudia, Vernieri Fabrizio
Headache and Neurosonology Unit, Neurology, Policlinico Campus Bio-Medico di Roma, Rome, Italy.
Stroke Unit, Medicina vascolare e d'urgenza, Università di Perugia, Perugia, Italy.
Front Neurol. 2017 Nov 27;8:624. doi: 10.3389/fneur.2017.00624. eCollection 2017.
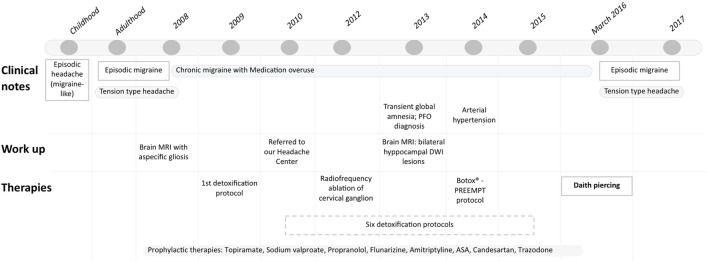
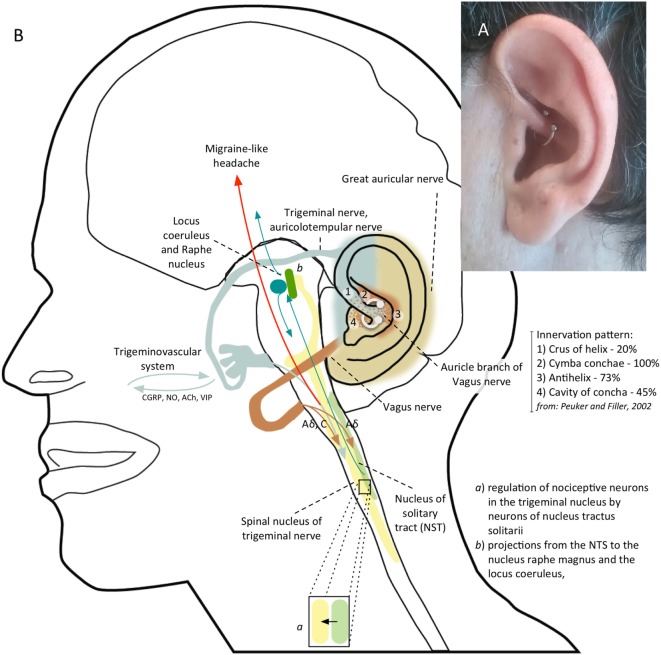
Daith piercing is an ear piercing located at the crus of the helix, bilaterally. It is getting great consent on social media as alternative treatment in chronic migraine. No data about its efficacy and action are available in scientific literature so far. We present the case of a 54-year-old male patient suffering from refractory chronic migraine with medication-overuse, who substantially improved after bilateral ear daith piercing. His migraine was refractory to symptomatic as well as prophylactic therapies. He used to treat headaches with up to five symptomatic drugs per attack and had attempted several pharmacological preventive therapies, including Onabotulinumtoxin A. He also underwent detoxification treatments with intravenous steroids and diazepam, without durable benefit. At the time of daith piercing, the headache-related disability measures showed a HIT-6 score of 64, a MIDAS-score of 70, and a 11-point Box scale of 5. On his own free will, he decided to get a "daith piercing." After that, he experienced a reduction of migraine attacks, which became very rare, and infrequent, less disabling episodes of tension-type headache (HIT-6 score of 56; MIDAS score of 27, 11-point Box scale of 3). Painkiller assumption has much decreased: he takes only one tablet of indomethacin 50 mg to treat tensive headaches, about four times per month. Beyond a placebo effect, we can speculate a vagal modulation as the action mechanism of daith piercing: a nociceptive sensory stimulus applied to trigeminal and vagal areas of the ear can activate ear vagal afferents, which can modulate pain pathways by means of projections to the caudal trigeminal nucleus, to the locus coeruleus and to the nucleus raphe magnus. Currently, daith piercing cannot be recommended as migraine treatment because of the lack of scientific evidence, the unquantified rate of failure and the associated risks with insertion. However, given the increasing but anecdotal evidence, we think that the mechanism needs testing by means of a controlled clinical trial in a population of chronic migraineurs.
戴氏穿孔术是一种在双侧耳轮脚处进行的耳部穿孔术。作为慢性偏头痛的替代治疗方法,它在社交媒体上获得了广泛认可。到目前为止,科学文献中尚无关于其疗效和作用的数据。我们报告一例54岁男性患者,患有难治性慢性偏头痛且药物滥用,双侧耳部戴氏穿孔术后病情显著改善。他的偏头痛对对症治疗和预防性治疗均无效。他每次发作时曾使用多达五种对症药物治疗头痛,并尝试过多种药物预防性治疗,包括A型肉毒杆菌毒素。他还接受了静脉注射类固醇和地西泮的解毒治疗,但没有持久疗效。在进行戴氏穿孔术时,与头痛相关的残疾评估显示,HIT-6评分为64分,MIDAS评分为70分,11点量表评分为5分。他出于自愿决定进行“戴氏穿孔术”。此后,他的偏头痛发作次数减少,变得非常罕见,紧张型头痛发作次数也减少且不那么致残(HIT-6评分为56分;MIDAS评分为27分,11点量表评分为3分)。止痛药的服用量大幅减少:他每月仅服用约四次50毫克吲哚美辛片来治疗紧张性头痛。除了安慰剂效应外,我们推测迷走神经调节是戴氏穿孔术的作用机制:施加于耳部三叉神经和迷走神经区域的伤害性感觉刺激可激活耳部迷走神经传入纤维,这些传入纤维可通过投射到三叉神经尾侧核、蓝斑和中缝大核来调节疼痛通路。目前,由于缺乏科学证据、失败率未量化以及穿孔相关风险,不建议将戴氏穿孔术作为偏头痛的治疗方法。然而,鉴于越来越多的轶事证据,我们认为需要通过对慢性偏头痛患者群体进行对照临床试验来检验其机制。