Feldthusen Anne-Dorthe, Larsen Jacob, Pedersen Palle L, Toft Kristensen Tina, Kvetny Jan
Department of Obstetrics & Gynaecology, Naestved Hospital, Ringstedgade 61, 4700 Naestved, Denmark.
The Mitochondrial Research Unit, Naestved Hospital, Ringstedgade 61, 4700 Naestved, Denmark.
J Clin Transl Endocrinol. 2013 Dec 24;1(1):e13-e17. doi: 10.1016/j.jcte.2013.12.003. eCollection 2014 Mar.
It is well documented that overt hypothyroidism is associated with adverse pregnancy outcomes, but studies of subclinical hypothyroidism have demonstrated conflicting results.
Thyroid hormones are known to regulate mitochondrial function, and the aim of this study was to examine the possible relationship of subclinical hypothyroidism and mitochondrial dysfunction to adverse pregnancy outcomes in pregnant women.
Women in their third trimester of pregnancy ( = 113) who did not receive thyroid medication were included in this cross-sectional study. All participants were interviewed, and their thyroid status was determined. All participants had concentrations of thyroid hormones (fT and tT) within the reference range. In addition to thyroid status, mitochondrial membrane potential (MMP) and reactive oxygen species (ROS) were measured by flow cytometry. To establish a reference range of MMP and ROS, a group of euthyroid, nonpregnant women were used as euthyroid controls. Adverse pregnancy outcome was defined as preterm delivery, preeclampsia, placental abruption, Apgar score <7 points 1 minute after birth, or postpartum hemorrhage.
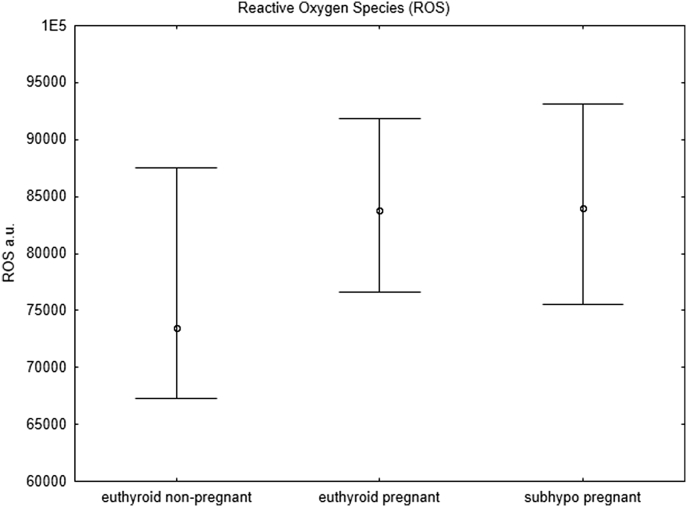
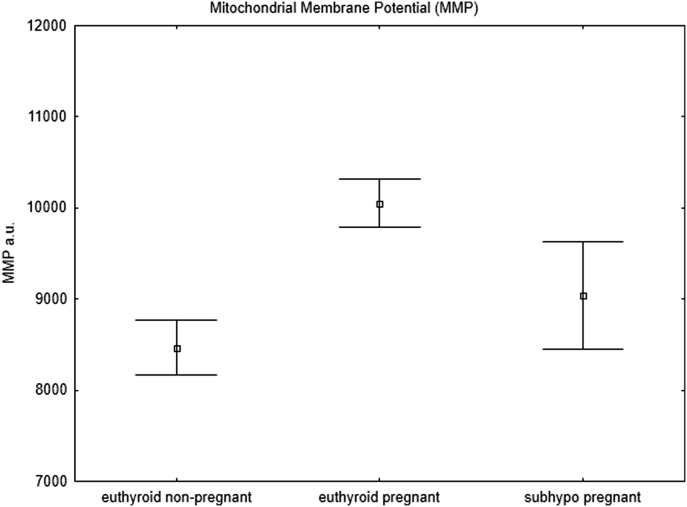
The prevalence of subclinical hypothyroidism among pregnant women was 17% ( = 19), and the number of overall adverse pregnancy outcomes was increased ( = 0.02) compared with that in euthyroid pregnant women. Preeclampsia, poor Apgar score, and postpartum hemorrhage were more frequent in the subclinical hypothyroidism group than in the euthyroid group ( = 0.04, = 0.001 and = 0.03, respectively), and more women showed prolonged gestation and gave birth later than 41 weeks of gestation than in the euthyroid group ( = 0.04). Compared with euthyroid, nonpregnant controls, a physiological upregulation of mitochondrial function was observed in euthyroid pregnant women. This was impaired in pregnant women with subclinical hypothyroidism. Compared with euthyroid, nonpregnant controls, pregnant women had increased ROS regardless of their thyroid status.
We speculate that the unfavorable effects on mitochondrial function in women with subclinical hypothyroidism may be associated with higher prevalence of adverse pregnancy outcomes.
有充分证据表明显性甲状腺功能减退与不良妊娠结局相关,但亚临床甲状腺功能减退的研究结果相互矛盾。
已知甲状腺激素可调节线粒体功能,本研究旨在探讨亚临床甲状腺功能减退和线粒体功能障碍与孕妇不良妊娠结局之间的可能关系。
本横断面研究纳入了113名未接受甲状腺药物治疗的孕晚期妇女。对所有参与者进行访谈,并确定其甲状腺状态。所有参与者的甲状腺激素(游离甲状腺素和总甲状腺素)浓度均在参考范围内。除甲状腺状态外,通过流式细胞术测量线粒体膜电位(MMP)和活性氧(ROS)。为建立MMP和ROS的参考范围,一组甲状腺功能正常的非孕妇被用作甲状腺功能正常的对照。不良妊娠结局定义为早产、先兆子痫、胎盘早剥、出生后1分钟阿氏评分<7分或产后出血。
孕妇中亚临床甲状腺功能减退的患病率为17%(19例),与甲状腺功能正常的孕妇相比,总体不良妊娠结局的数量增加(P=0.02)。亚临床甲状腺功能减退组先兆子痫、阿氏评分低和产后出血的发生率高于甲状腺功能正常组(分别为P=0.04、P=0.001和P=0.03),与甲状腺功能正常组相比,更多妇女出现妊娠期延长并在妊娠41周后分娩(P=0.04)。与甲状腺功能正常的非孕妇对照相比,甲状腺功能正常的孕妇中线粒体功能出现生理性上调。而亚临床甲状腺功能减退的孕妇中这种上调受到损害。与甲状腺功能正常的非孕妇对照相比,无论甲状腺状态如何,孕妇的ROS均增加。
我们推测亚临床甲状腺功能减退女性线粒体功能的不利影响可能与不良妊娠结局的较高发生率有关。