Division of Cardiovascular Medicine, Radcliffe Department of Medicine, BHF Centre of Research Excellence at the University of Oxford and the Wellcome Trust Centre for Human Genetics, Roosevelt Drive, Oxford OX3 7BN, UK.
German Centre for Cardiovascular Research (DZHK), Partner Site Munich Heart Alliance, Institute for Cardiovascular Prevention (IPEK), Pettenkoferstraße 8a & 9, 80336 Munich, Germany.
Cardiovasc Res. 2018 Mar 1;114(3):417-430. doi: 10.1093/cvr/cvx242.
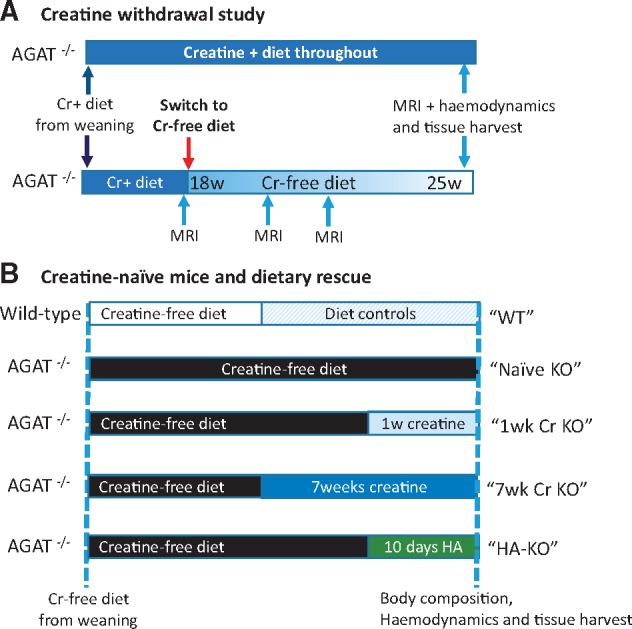
Creatine buffers cellular adenosine triphosphate (ATP) via the creatine kinase reaction. Creatine levels are reduced in heart failure, but their contribution to pathophysiology is unclear. Arginine:glycine amidinotransferase (AGAT) in the kidney catalyses both the first step in creatine biosynthesis as well as homoarginine (HA) synthesis. AGAT-/- mice fed a creatine-free diet have a whole body creatine-deficiency. We hypothesized that AGAT-/- mice would develop cardiac dysfunction and rescue by dietary creatine would imply causality.
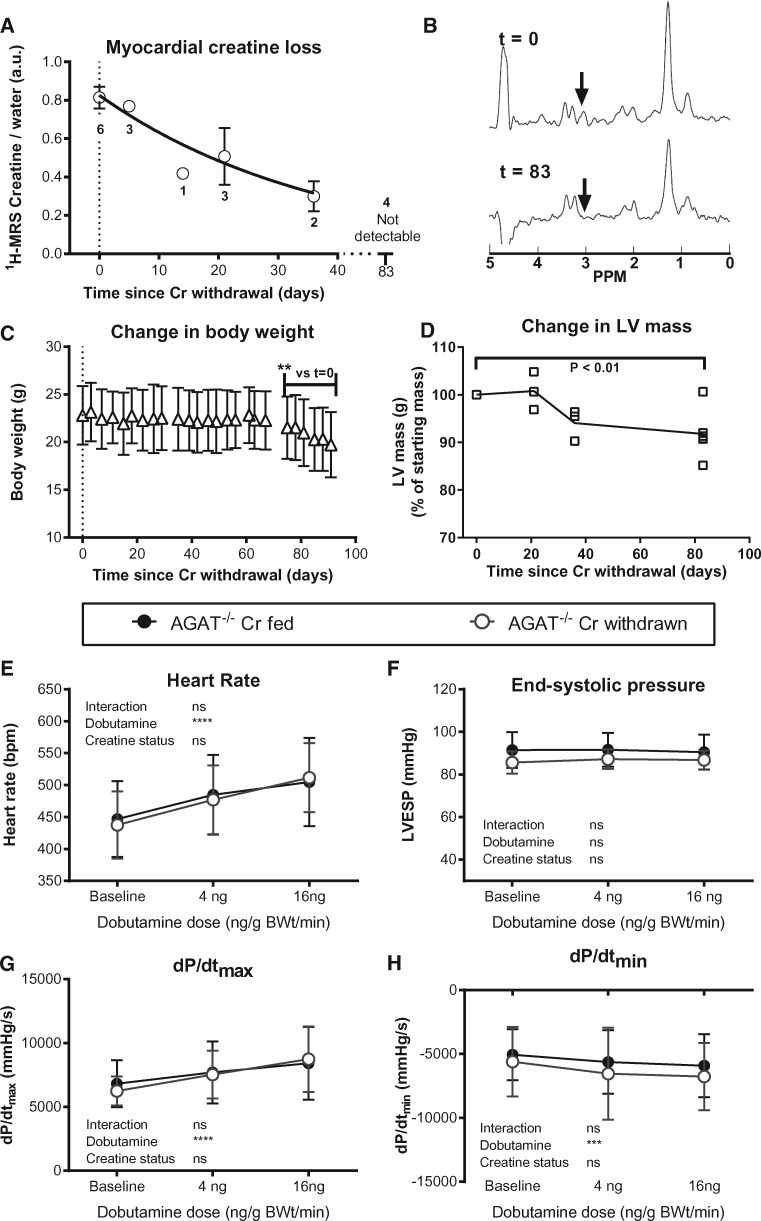
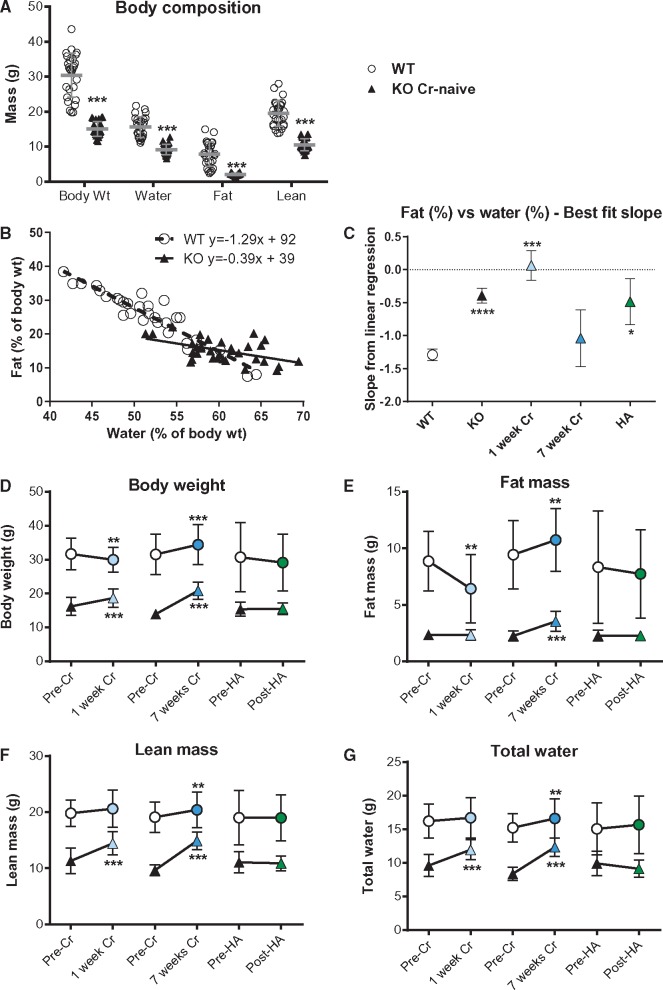
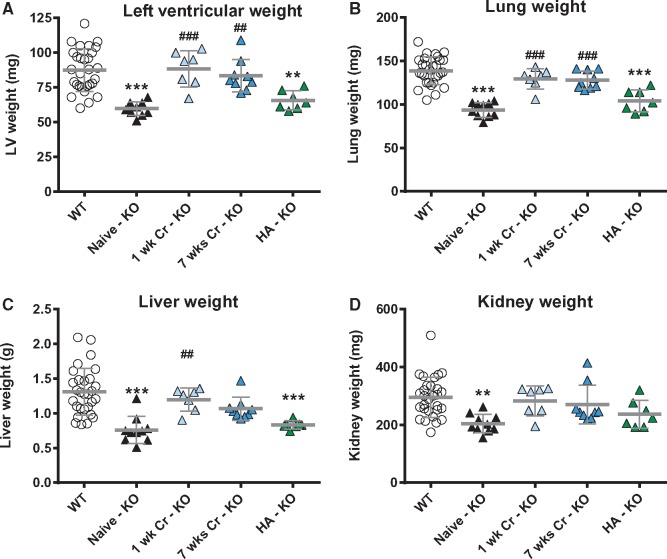
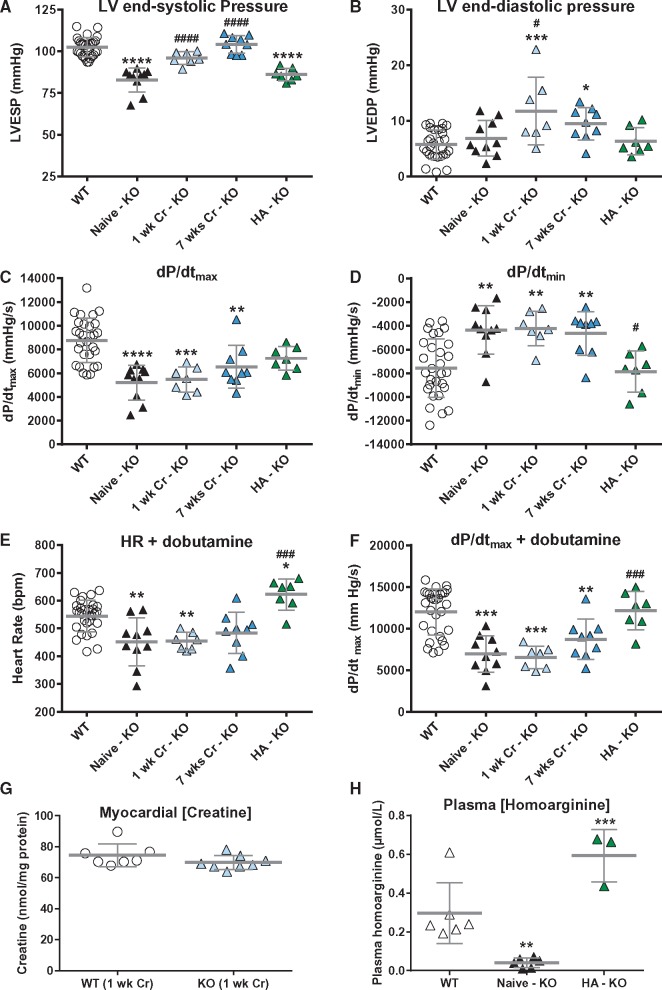
Withdrawal of dietary creatine in AGAT-/- mice provided an estimate of myocardial creatine efflux of ∼2.7%/day; however, in vivo cardiac function was maintained despite low levels of myocardial creatine. Using AGAT-/- mice naïve to dietary creatine we confirmed absence of phosphocreatine in the heart, but crucially, ATP levels were unchanged. Potential compensatory adaptations were absent, AMPK was not activated and respiration in isolated mitochondria was normal. AGAT-/- mice had rescuable changes in body water and organ weights suggesting a role for creatine as a compatible osmolyte. Creatine-naïve AGAT-/- mice had haemodynamic impairment with low LV systolic pressure and reduced inotropy, lusitropy, and contractile reserve. Creatine supplementation only corrected systolic pressure despite normalization of myocardial creatine. AGAT-/- mice had low plasma HA and supplementation completely rescued all other haemodynamic parameters. Contractile dysfunction in AGAT-/- was confirmed in Langendorff perfused hearts and in creatine-replete isolated cardiomyocytes, indicating that HA is necessary for normal cardiac function.
Our findings argue against low myocardial creatine per se as a major contributor to cardiac dysfunction. Conversely, we show that HA deficiency can impair cardiac function, which may explain why low HA is an independent risk factor for multiple cardiovascular diseases.
肌酸通过肌酸激酶反应缓冲细胞三磷酸腺苷 (ATP)。心力衰竭时肌酸水平降低,但它们对病理生理学的贡献尚不清楚。肾脏中的精氨酸:甘氨酸酰胺转移酶 (AGAT) 催化肌酸生物合成的第一步以及同型精氨酸 (HA) 的合成。在喂食无肌酸饮食的 AGAT-/- 小鼠中,全身肌酸缺乏。我们假设 AGAT-/- 小鼠会出现心脏功能障碍,而饮食肌酸的挽救作用则表明存在因果关系。
AGAT-/- 小鼠停止饮食肌酸提供了心肌肌酸外排率约为 2.7%/天的估计值;然而,尽管心肌肌酸水平较低,体内心脏功能仍得以维持。我们使用对饮食肌酸不熟悉的 AGAT-/- 小鼠证实了心脏中不存在磷酸肌酸,但至关重要的是,ATP 水平保持不变。缺乏潜在的代偿适应,AMPK 未被激活,分离线粒体的呼吸正常。AGAT-/- 小鼠的身体水分和器官重量有可挽救的变化,这表明肌酸作为一种相容的渗透调节剂具有作用。缺乏肌酸的 AGAT-/- 小鼠有血液动力学受损,左心室收缩压降低,变力性、松弛性和收缩储备降低。尽管心肌肌酸正常化,但肌酸补充仅纠正了收缩压。AGAT-/- 小鼠的血浆 HA 水平较低,补充剂完全挽救了所有其他血液动力学参数。在 Langendorff 灌注心脏和肌酸充足的分离心肌细胞中证实了 AGAT-/- 的收缩功能障碍,表明 HA 是心脏正常功能所必需的。
我们的发现表明,心肌肌酸本身水平降低不是导致心脏功能障碍的主要原因。相反,我们表明 HA 缺乏会损害心脏功能,这可能解释了为什么低 HA 是多种心血管疾病的独立危险因素。