Ravvaz Kourosh, Weissert John A, Ruff Christian T, Chi Chih-Lin, Tonellato Peter J
From the Aurora Research Institute, Aurora Health Care, Milwaukee, WI (K.R., J.A.W.); Brigham and Women's Hospital, Harvard Medical School, Boston, MA (C.T.R., P.J.T.); School of Nursing and Institute for Health Informatics, University of Minnesota, Minneapolis (C.-L.C.); and University of Wisconsin, Milwaukee (P.J.T.).
Circ Cardiovasc Genet. 2017 Dec;10(6). doi: 10.1161/CIRCGENETICS.117.001804.
Clinical trials testing pharmacogenomic-guided warfarin dosing for patients with atrial fibrillation have demonstrated conflicting results. Non-vitamin K antagonist oral anticoagulants are expensive and contraindicated for several conditions. A strategy optimizing anticoagulant selection remains an unmet clinical need.
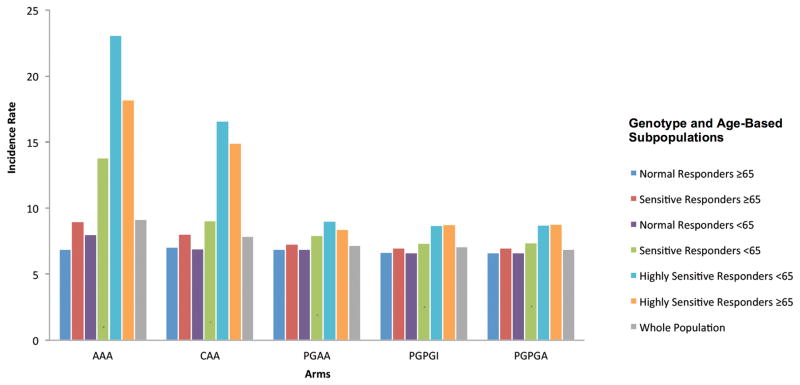
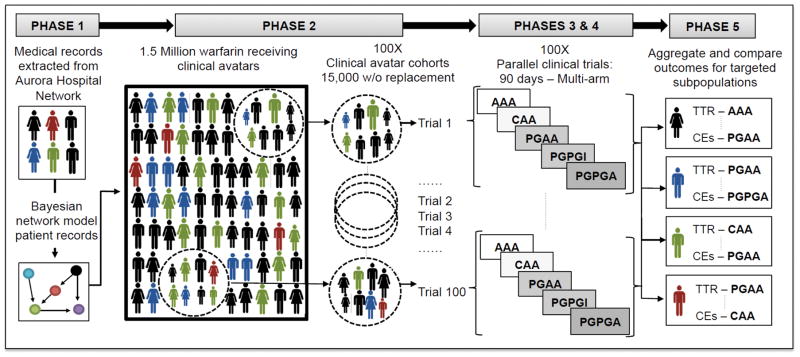
Characteristics from 14 206 patients with atrial fibrillation were integrated into a validated warfarin clinical trial simulation framework using iterative Bayesian network modeling and a pharmacokinetic-pharmacodynamic model. Individual dose-response for patients was simulated for 5 warfarin protocols-a fixed-dose protocol, a clinically guided protocol, and 3 increasingly complex pharmacogenomic-guided protocols. For each protocol, a complexity score was calculated using the variables predicting warfarin dose and the number of predefined international normalized ratio (INR) thresholds for each adjusted dose. Study outcomes included optimal time in therapeutic range ≥65% and clinical events. A combination of age and genotype identified different optimal protocols for various subpopulations. A fixed-dose protocol provided well-controlled INR only in normal responders ≥65, whereas for normal responders <65 years old, a clinically guided protocol was necessary to achieve well-controlled INR. Sensitive responders ≥65 and <65 and highly sensitive responders ≥65 years old required pharmacogenomic-guided protocols to achieve well-controlled INR. However, highly sensitive responders <65 years old did not achieve well-controlled INR and had higher associated clinical events rates than other subpopulations.
Under the assumptions of this simulation, patients with atrial fibrillation can be triaged to an optimal warfarin therapy protocol by age and genotype. Clinicians should consider alternative anticoagulation therapy for patients with suboptimal outcomes under any warfarin protocol.
针对心房颤动患者进行的药物基因组学指导华法林剂量的临床试验结果相互矛盾。非维生素K拮抗剂口服抗凝剂价格昂贵,且在多种情况下禁用。优化抗凝剂选择的策略仍是未满足的临床需求。
利用迭代贝叶斯网络建模和药代动力学-药效学模型,将14206例心房颤动患者的特征整合到经过验证的华法林临床试验模拟框架中。针对5种华法林方案模拟了患者的个体剂量反应,这5种方案分别是固定剂量方案、临床指导方案以及3种越来越复杂的药物基因组学指导方案。对于每种方案,使用预测华法林剂量的变量和每个调整剂量的预定义国际标准化比值(INR)阈值数量计算复杂性评分。研究结果包括治疗范围内的最佳时间≥65%以及临床事件。年龄和基因型的组合为不同亚组确定了不同的最佳方案。固定剂量方案仅在年龄≥65岁的正常反应者中能实现INR的良好控制,而对于年龄<65岁的正常反应者,需要临床指导方案才能实现INR的良好控制。年龄≥65岁和<65岁的敏感反应者以及年龄≥65岁的高敏反应者需要药物基因组学指导方案来实现INR的良好控制。然而,年龄<65岁的高敏反应者未实现INR的良好控制,且与其他亚组相比临床事件发生率更高。
在本模拟的假设下,心房颤动患者可根据年龄和基因型分类至最佳华法林治疗方案。对于在任何华法林方案下预后不佳的患者,临床医生应考虑替代抗凝治疗。