Gruzdeva Olga, Uchasova Evgenya, Dyleva Yulia, Akbasheva Olga, Karetnikova Victoria, Shilov Aleksandr, Barbarash Olga
Federal State Budgetary Institution, Research Institute for Complex Issues of Cardiovascular Diseases, Kemerovo, Russia.
State Budget Educational Institution of Higher Professional Education, Siberian State Medical University, Russian Federation Ministry of Health, Tomsk, Russia.
Diabetes Metab Syndr Obes. 2017 Dec 5;10:481-489. doi: 10.2147/DMSO.S149463. eCollection 2017.
Cardiovascular diseases and type 2 diabetes mellitus (T2DM) may have common developmental mechanisms associated with lipid metabolism disorders. Dyslipidemia and progression of atherosclerosis in people with T2DM are accompanied by an increase in cardiovascular mortality. This study examined the dose-dependent action of atorvastatin on carbohydrate metabolism and adipokine status in patients within 12 months after myocardial infarction (MI).
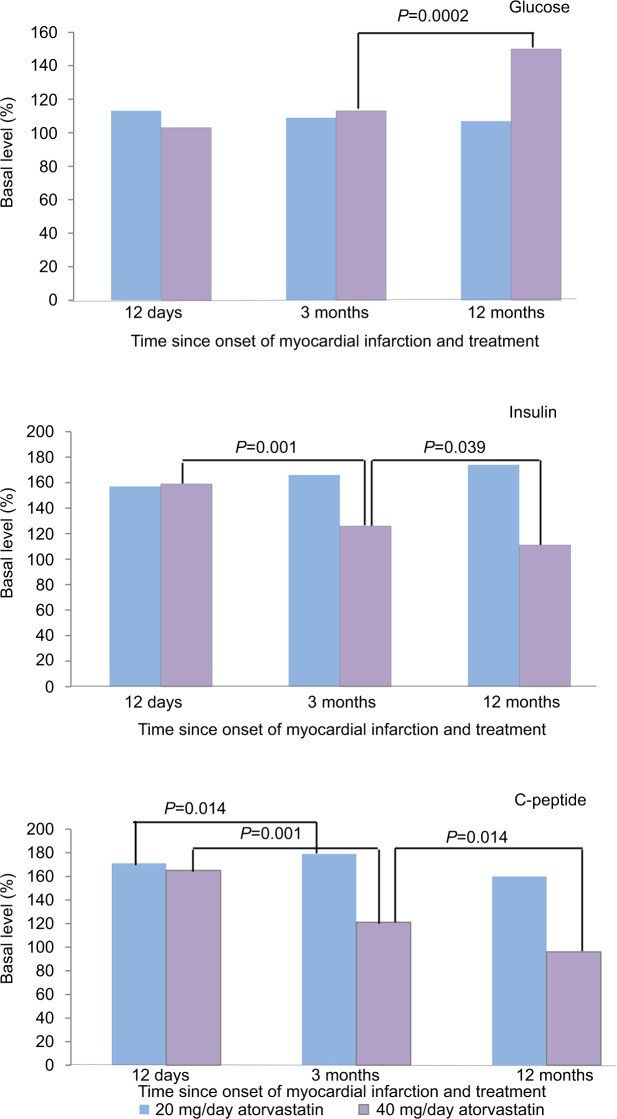
A total of 156 male MI patients who had received atorvastatin 20 mg/day (78 patients) or 40 mg/day (78 patients) starting from day 1 of onset were enrolled. Glucose, insulin, C-peptide, resistin, adiponectin, and ghrelin levels were measured at baseline, day 12, and months 3 and 12. Patients were monitored for new incidences of T2DM for 12 months after MI.
For acute phase MI, patients had moderate insulin resistance, hyperglycemia, and hyper-insulinemia, high leptin and resistin levels, and low ghrelin and adiponectin levels. Atorvastatin 20 mg/day was more effective at correcting the imbalances. Patients taking atorvastatin 40 mg/day (group 2) following MI showed increases in levels of glucose, insulin, and C-peptide and insulin resistance progression after 12 months of therapy, as evidenced by increased quantitative insulin sensitivity check index scores and detection of new T2DM cases.
Atorvastatin improved adipokine profiles and ghrelin levels, with low doses showing more significant effects. Atorvastatin dose prescribed for MI patients should take into account the degree of insulin resistance and adipokine status.
心血管疾病和2型糖尿病(T2DM)可能具有与脂质代谢紊乱相关的共同发病机制。T2DM患者的血脂异常和动脉粥样硬化进展伴随着心血管死亡率的增加。本研究调查了阿托伐他汀对心肌梗死(MI)后12个月内患者碳水化合物代谢和脂肪因子状态的剂量依赖性作用。
总共纳入156名男性MI患者,这些患者自发病第1天起接受20毫克/天(78例患者)或40毫克/天(78例患者)的阿托伐他汀治疗。在基线、第12天、第3个月和第12个月时测量血糖、胰岛素、C肽、抵抗素、脂联素和胃饥饿素水平。在MI后对患者进行12个月的T2DM新发病例监测。
对于急性期MI患者,存在中度胰岛素抵抗、高血糖和高胰岛素血症,瘦素和抵抗素水平高,胃饥饿素和脂联素水平低。20毫克/天的阿托伐他汀在纠正失衡方面更有效。MI后服用40毫克/天阿托伐他汀的患者(第2组)在治疗12个月后血糖、胰岛素和C肽水平升高,胰岛素抵抗进展,定量胰岛素敏感性检查指数评分增加以及新的T2DM病例检测证明了这一点。
阿托伐他汀改善了脂肪因子谱和胃饥饿素水平,低剂量显示出更显著的效果。为MI患者开具的阿托伐他汀剂量应考虑胰岛素抵抗程度和脂肪因子状态。