Department of Otolaryngology-Head and Neck Surgery, University of Michigan Health Center, Ann Arbor, MI, USA.
Department of Biostatistics, University of Michigan Health Center, Ann Arbor, MI, USA.
Ann Surg Oncol. 2018 May;25(5):1288-1295. doi: 10.1245/s10434-017-6278-4. Epub 2017 Dec 20.
Patients undergoing salvage laryngectomy are predisposed to radiation-induced hypothyroidism and impaired wound healing secondary to the tissue effects of prior treatment. The impact of hypothyroidism on postoperative wound healing is not established.
A single-institution retrospective case series was performed. The inclusion criteria specified preoperatively euthyroid adults who underwent salvage laryngectomy with concurrent neck dissection between 1997 and 2015 for persistent or recurrent laryngeal squamous cell carcinoma after radiation or chemoradiation therapy (n = 182). The principal explanatory variable was postoperative hypothyroidism, defined as thyroid-stimulating hormone (TSH) higher than 5.5 mIU/L. The primary end points of the study were pharyngocutaneous fistulas and wounds requiring reoperation. Multivariate analysis was performed.
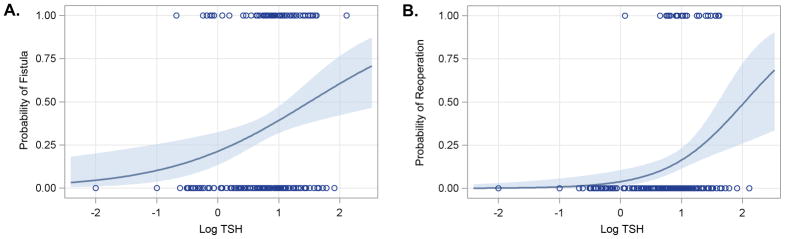
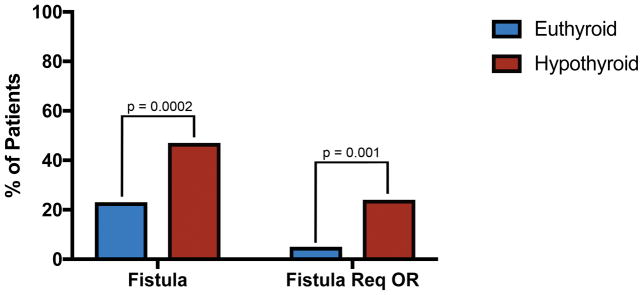
The fistula rate was 47% among hypothyroid patients versus 23% among euthyroid patients. In the multivariate analysis, the patients who experienced hypothyroidism in the postoperative period had a 3.6-fold greater risk of fistula [95% confidence interval (CI) 1.8-7.1; p = 0.0002]. The hypothyroid patients had an 11.4-fold greater risk for a required reoperation (24.4 vs 5.4%) than the euthyroid patients (95% CI 2.6-49.9; p = 0.001). The risk for fistula (p = 0.003) and reoperation (p = 0.001) increased with increasing TSH. This corresponds to an approximate 12.5% incremental increase in the absolute risk for fistula and a 10% increase in the absolute risk for reoperation with each doubling of the TSH.
Postoperative hypothyroidism independently predicts postoperative wound-healing complications. The association of hypothyroidism with fistula formation may yield opportunities to modulate wound healing with thyroid supplementation or to provide a biomarker of wound progression.
接受挽救性喉切除术的患者由于先前治疗的组织效应,容易发生放射性甲状腺功能减退症和伤口愈合受损。甲状腺功能减退症对术后伤口愈合的影响尚未确定。
进行了一项单机构回顾性病例系列研究。纳入标准为 1997 年至 2015 年间因放疗或放化疗后持续性或复发性喉鳞状细胞癌而接受挽救性喉切除术和同期颈部清扫术的术前甲状腺功能正常的成年人(n=182)。主要解释变量为术后甲状腺功能减退症,定义为促甲状腺激素(TSH)高于 5.5 mIU/L。该研究的主要终点为咽皮瘘和需要再次手术的伤口。进行了多变量分析。
甲状腺功能减退症患者的瘘管发生率为 47%,而甲状腺功能正常的患者为 23%。在多变量分析中,术后发生甲状腺功能减退症的患者发生瘘管的风险增加 3.6 倍[95%置信区间(CI)1.8-7.1;p=0.0002]。甲状腺功能减退症患者需要再次手术的风险比甲状腺功能正常的患者高 11.4 倍(24.4%比 5.4%)(95%CI 2.6-49.9;p=0.001)。瘘管(p=0.003)和再次手术(p=0.001)的风险随着 TSH 的增加而增加。这相当于瘘管的绝对风险增加约 12.5%,TSH 每增加一倍,再次手术的绝对风险增加 10%。
术后甲状腺功能减退症独立预测术后伤口愈合并发症。甲状腺功能减退症与瘘管形成的关联可能为通过甲状腺素补充来调节伤口愈合提供机会,或为伤口进展提供生物标志物。