Beddhu Srinivasan, Wei Guo, Chen Xiaorui, Boucher Robert, Kiani Rabia, Raj Dominic, Chonchol Michel, Greene Tom, Murtaugh Maureen A
VA Healthcare System, Salt Lake City, Utah, USA.
Department of Medicine, University of Utah School of Medicine, Salt Lake City, Utah, USA.
Kidney Int Rep. 2017 Apr 18;2(5):821-830. doi: 10.1016/j.ekir.2017.04.002. eCollection 2017 Sep.
The associations of dietary protein and/or energy intakes with protein or energy wasting in patients on maintenance hemodialysis are controversial. We examined these in the Hemodialysis (HEMO) Study.
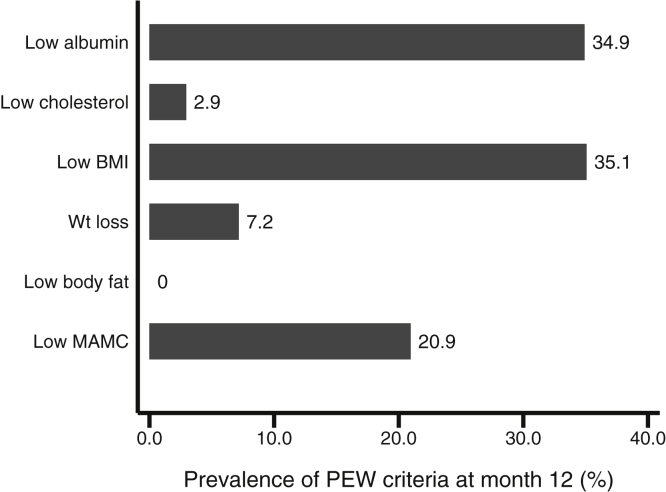
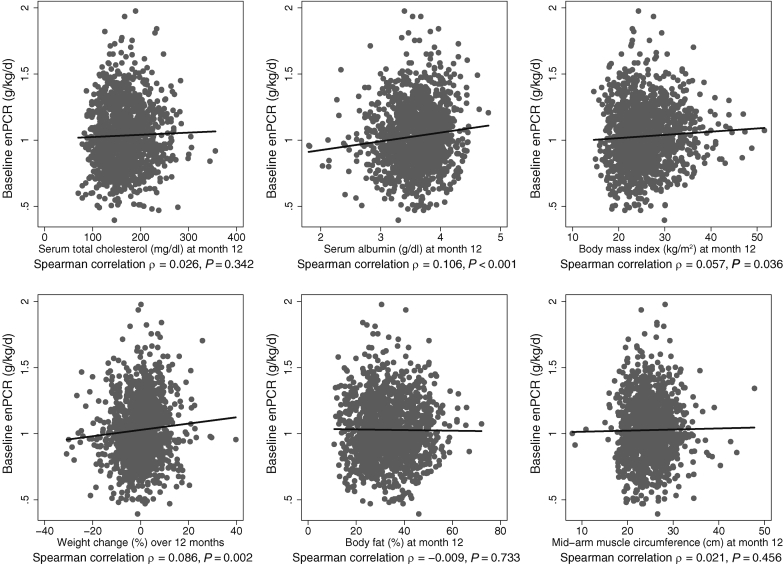
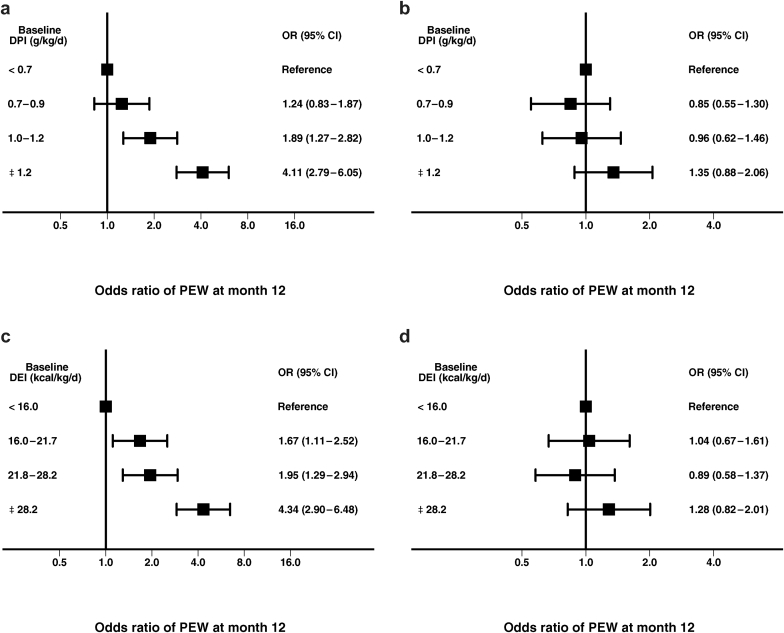
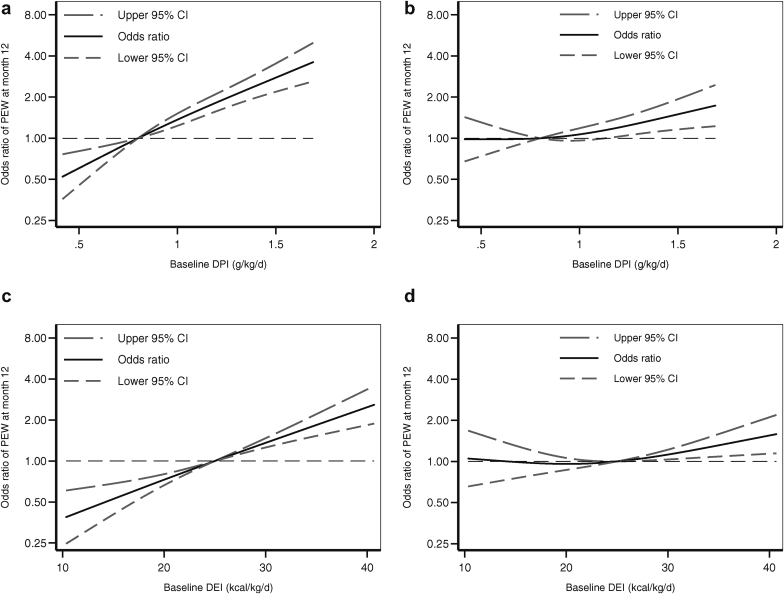
In 1487 participants in the HEMO Study, baseline dietary protein intake (grams per kilogram per day) and dietary energy intake (kilocalories per kilograms per day) were related to the presence of the protein-energy wasting (PEW) syndrome at month 12 (defined as the presence of at least 1 criteria in 2 of the 3 categories of low serum chemistry, low body mass, and low muscle mass) in logistic regression models. In additional separate models, protein intake estimated from equilibrated normalized protein catabolic rate (enPCR) was also related to the PEW syndrome.
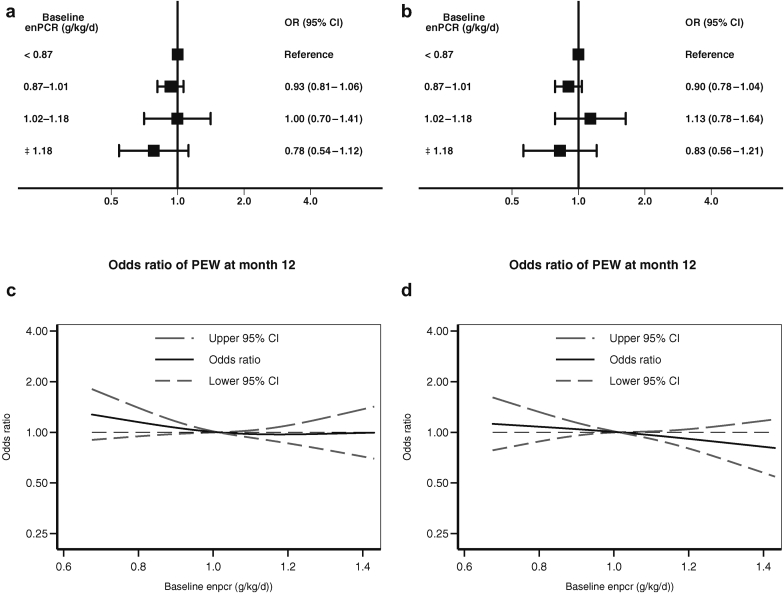
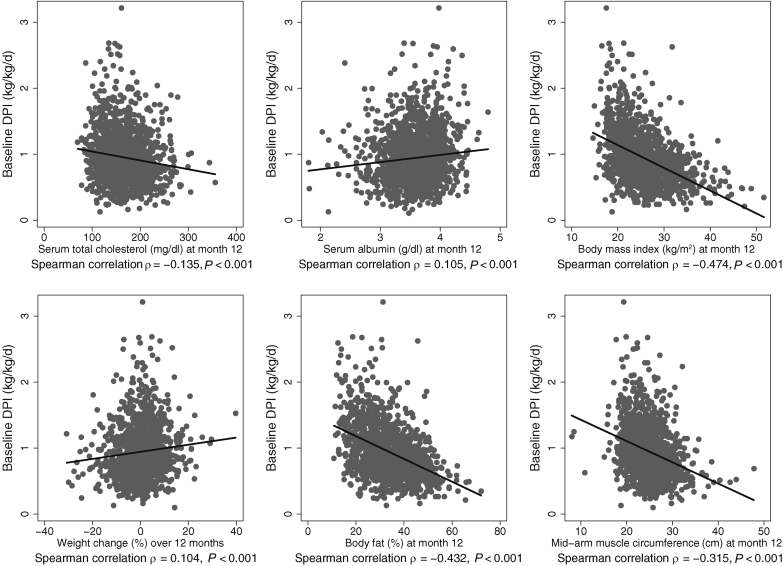
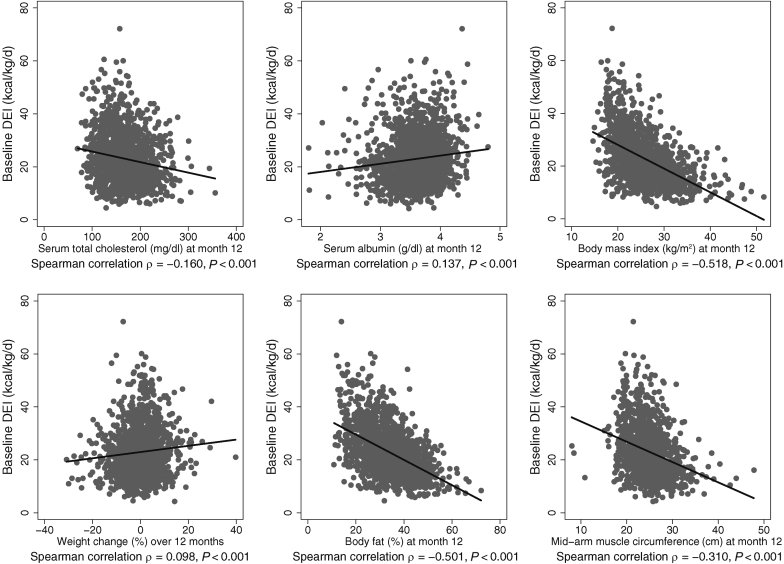
Compared with the lowest quartile, the highest quartile of baseline dietary protein intake was paradoxically associated with increased risk of the PEW syndrome at month 12 (odds ratio [OR]: 4.11; 95% confidence interval [CI]: 2.79-6.05). This relationship was completely attenuated (OR: 1.35; 95% CI: 0.88-2.06) with adjustment for baseline body weight, which suggested mathematical coupling. Results were similar for dietary energy intake. Compared with the lowest quartile of baseline enPCR, the highest quartile was not associated with the PEW syndrome at 12 months (OR: 0.78; 95% CI: 0.54-1.12).
These data do not support the use of dietary protein intake or dietary energy intake criteria in the definition of the PEW syndrome in patients on maintenance hemodialysis.
维持性血液透析患者的膳食蛋白质和/或能量摄入与蛋白质或能量消耗之间的关联存在争议。我们在血液透析(HEMO)研究中对此进行了调查。
在HEMO研究的1487名参与者中,在逻辑回归模型中,将基线膳食蛋白质摄入量(克/千克/天)和膳食能量摄入量(千卡/千克/天)与第12个月时蛋白质-能量消耗(PEW)综合征的存在情况(定义为在低血清化学、低体重和低肌肉量这3类中的2类中至少存在1条标准)相关联。在另外单独的模型中,根据平衡归一化蛋白质分解代谢率(enPCR)估算的蛋白质摄入量也与PEW综合征相关。
与最低四分位数相比,基线膳食蛋白质摄入量的最高四分位数与第12个月时PEW综合征风险增加存在矛盾关联(比值比[OR]:4.11;95%置信区间[CI]:2.79 - 6.05)。在对基线体重进行调整后,这种关系完全减弱(OR:1.35;95% CI:0.88 - 2.06),这表明存在数学上的耦合。膳食能量摄入的结果类似。与基线enPCR的最低四分位数相比,最高四分位数在12个月时与PEW综合征无关(OR:0.78;95% CI:0.54 - 1.12)。
这些数据不支持在定义维持性血液透析患者的PEW综合征时使用膳食蛋白质摄入量或膳食能量摄入量标准。