Overlook Medical Center, Columbia University College of Physicians and Surgeons, New York, NY, USA.
, 11 Overlook Rd Suite 160, Summit, NJ, 07901, USA.
Surg Endosc. 2018 Mar;32(3):1586-1592. doi: 10.1007/s00464-017-6001-3. Epub 2017 Dec 22.
The PILLAR II trial demonstrated PINPOINT is safe, feasible to use with no reported adverse events and resulted in no anastomotic leaks in patients who had a change in surgical plan based on PINPOINT's intraoperative assessment of tissue perfusion during colorectal resection. Whether the cost savings associated with this reduction in anastomotic complications can offset the cost of investing in PINPOINT is unknown.
We performed a retrospective analysis of all patients (N = 347) undergoing colectomy with primary anastomosis from January 2015 to April 2016. These patients were stratified based on whether fluorescence imaging was used intraoperatively. The clinical outcomes of these patients were then evaluated based on their development of an anastomotic leak or stricture. The direct hospital costs per case were then calculated, and the economic impact of using fluorescence imaging was examined to assess whether decreased direct costs would justify the initial expenditures to purchase new technology (PINPOINT System, NOVADAQ, Canada).
Fluorescence imaging in colorectal surgery using PINPOINT reduced the anastomotic failure rate in patients who underwent colon resection. The PINPOINT group (n = 238) had two (0.84%) anastomotic failures, while the non-PINPOINT group (n = 109) had six (5.5%) anastomotic failures. In the PINPOINT group, 11 (4.6%) patients had a change in the resection margin based on the results of the fluorescence imaging, and none of these patients experienced an anastomotic failure. Cost per case was less in the PINPOINT group secondary to fewer direct costs associated with complications.
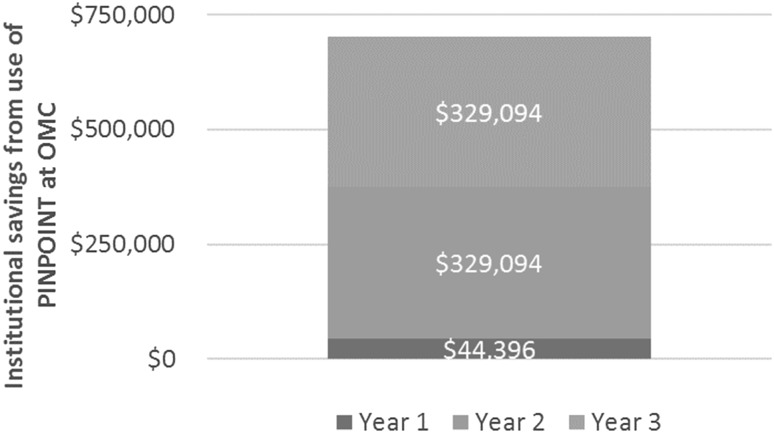
These results validate the findings of the PILLAR II trial and confirm the decrease in direct costs due to reduction in anastomotic failures as a result of using PINPOINT justified the expense of the new technology after just 143 cases.
PILLAR II 试验表明,PINPOINT 使用安全,可行,没有报告不良事件,并且在根据 PINPOINT 在结直肠切除术中对组织灌注的术中评估改变手术计划的患者中没有吻合口漏。是否可以通过减少吻合口并发症相关的成本节省来抵消投资 PINPOINT 的成本尚不清楚。
我们对 2015 年 1 月至 2016 年 4 月期间接受原发性吻合术的所有患者(N=347)进行了回顾性分析。这些患者根据术中是否使用荧光成像进行分层。然后根据吻合口漏或狭窄的发生评估这些患者的临床结果。然后计算每个病例的直接医院费用,并检查荧光成像的经济影响,以评估降低直接成本是否可以证明购买新技术(PINPOINT 系统,NOVADAQ,加拿大)的初始支出是合理的。
在结直肠手术中使用 PINPOINT 的荧光成像降低了接受结肠切除术的患者的吻合口失败率。PINPOINT 组(n=238)有两例(0.84%)吻合口失败,而非 PINPOINT 组(n=109)有六例(5.5%)吻合口失败。在 PINPOINT 组中,有 11 例(4.6%)患者因荧光成像结果改变了切除范围,且这些患者均未发生吻合口失败。PINPOINT 组的每个病例的成本较低,因为与并发症相关的直接成本较低。
这些结果验证了 PILLAR II 试验的结果,并证实了由于使用 PINPOINT 减少吻合口失败导致的直接成本降低,在仅仅 143 例患者后就证明了新技术的费用是合理的。