South Charles, Rush A John, Carmody Thomas J, Jha Manish K, Trivedi Madhukar H
Center for Depression Research and Clinical Care.
Department of Psychiatry.
Neuropsychiatr Dis Treat. 2017 Dec 15;13:3001-3010. doi: 10.2147/NDT.S139577. eCollection 2017.
The objective of the study was to determine whether a unique analytic approach - as a proof of concept - could identify individual depressed outpatients (using 30 baseline clinical and demographic variables) who are very likely (75% certain) to not benefit (NB) or to remit (R), accepting that without sufficient certainty, no prediction (NP) would be made.
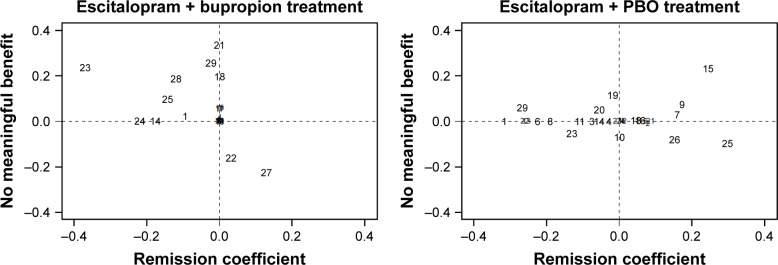
Patients from the Combining Medications to Enhance Depression Outcomes trial treated with escitalopram (S-CIT) + placebo (n=212) or S-CIT + bupropion-SR (n=206) were analyzed separately to assess replicability. For each treatment, the elastic net was used to identify subsets of predictive baseline measures for R and NB, separately. Two different equations that estimate the likelihood of remission and no benefit were developed for each patient. The ratio of these two numbers characterized likely outcomes for each patient.
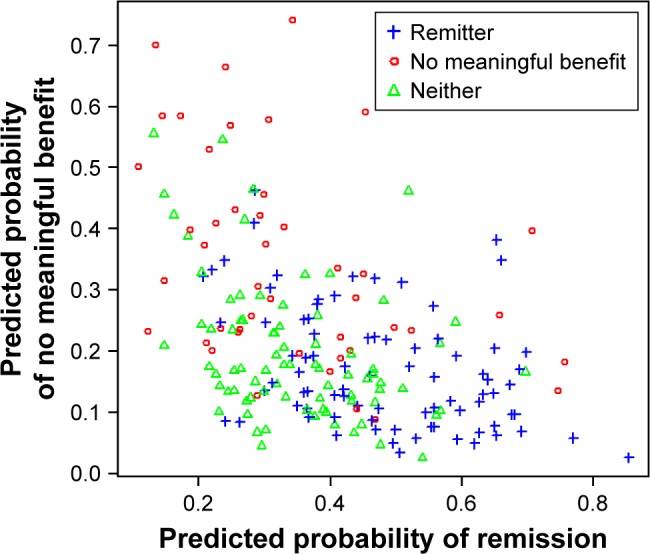
The two treatment cells had comparable rates of remission (40%) and no benefit (22%). In S-CIT + bupropion-SR, 11 were predicted NB of which 82% were correct; 26 were predicted R - 85% correct (169 had NP). For S-CIT + placebo, 13 were predicted NB - 69% correct; 44 were predicted R - 75% correct (155 were NP). Overall, 94/418 (22%) patients were identified with a meaningful degree of certainty (69%-85% correct). Different variable sets with some overlap were predictive of remission and no benefit within and across treatments, despite comparable outcomes.
In two separate analyses with two different treatments, this analytic approach - which is also applicable to pretreatment laboratory tests - identified a meaningful proportion (over 20%) of depressed patients for whom a treatment outcome was predicted with sufficient certainty that the clinician can elect to strongly recommend for or choose to avoid a particular treatment. Different persons seem to be remitting or not benefiting with these two different treatments.
本研究的目的是确定一种独特的分析方法——作为概念验证——能否识别出极有可能(75%确定)无获益(NB)或缓解(R)的个体抑郁症门诊患者(使用30个基线临床和人口统计学变量),前提是如果没有足够的确定性,就不进行预测(NP)。
对来自“联合用药改善抑郁结局”试验中接受艾司西酞普兰(S-CIT)+安慰剂(n = 212)或S-CIT +安非他酮缓释剂(n = 206)治疗的患者分别进行分析,以评估可重复性。对于每种治疗,弹性网络分别用于识别预测缓解和无获益的基线测量子集。为每位患者开发了两个不同的方程,分别估计缓解和无获益的可能性。这两个数字的比值表征了每位患者可能的结局。
两个治疗组的缓解率(40%)和无获益率(22%)相当。在S-CIT +安非他酮缓释剂组中,预测为NB的有11例,其中82%预测正确;预测为R的有26例——85%预测正确(169例为NP)。对于S-CIT +安慰剂组,预测为NB的有13例——69%预测正确;预测为R的有44例——75%预测正确(155例为NP)。总体而言,94/418(22%)例患者被确定具有有意义程度的确定性(69%-85%正确)。尽管结局相当,但不同治疗组内和不同治疗组间,有一些重叠的不同变量集可预测缓解和无获益。
在两项分别采用两种不同治疗方法的分析中,这种分析方法——也适用于治疗前实验室检查——识别出了相当比例(超过20%)的抑郁症患者,对于这些患者,治疗结局的预测具有足够的确定性,临床医生可以选择强烈推荐或选择避免某种特定治疗。不同的患者似乎对这两种不同的治疗有缓解或无获益的差异。