From the Department of Anesthesiology and Perioperative Medicine, Division of Critical Care Medicine, Mayo Clinic, Rochester, Minnesota.
Internal Medicine, Mount Auburn Hospital, Harvard Medical School, Cambridge, Massachusetts.
Anesth Analg. 2019 Feb;128(2):288-295. doi: 10.1213/ANE.0000000000002794.
Thrombocytopenia is frequently encountered in critically ill patients, often resulting in prophylactic transfusion of platelets for the prevention of bleeding complications. However, the efficacy of this practice remains unclear. The objective of this study was to determine the relationship between prophylactic platelet transfusion and bleeding complications in critically ill patients.
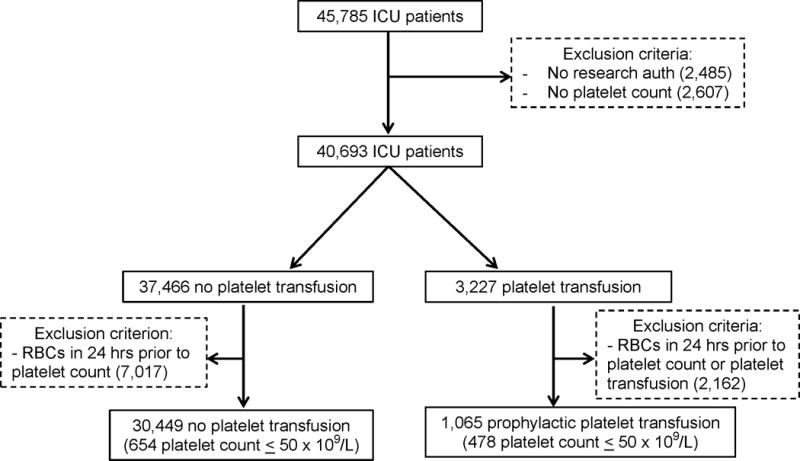
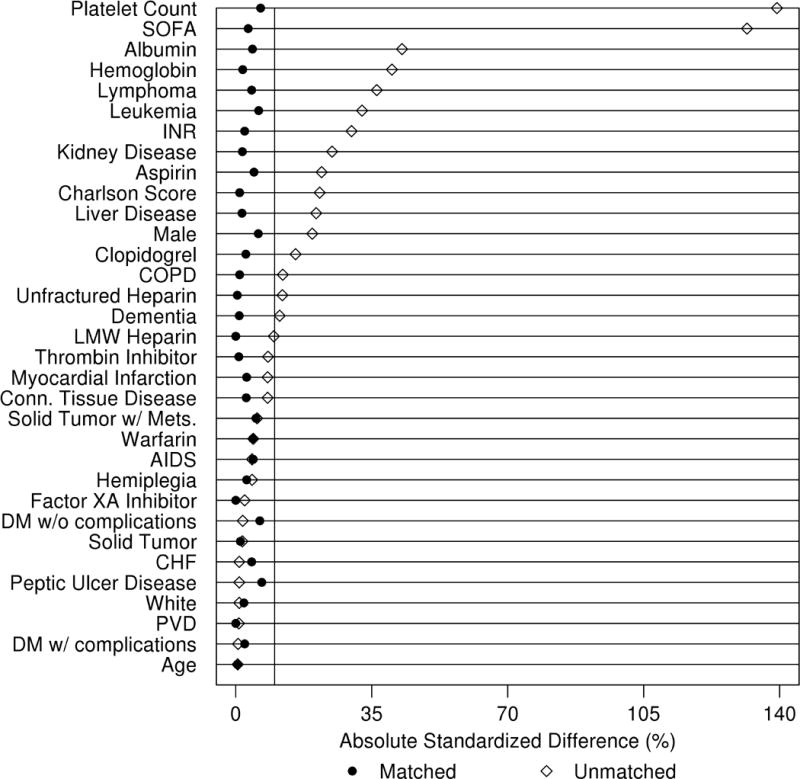
This is a retrospective cohort study of adults admitted to surgical, medical, or combined medical-surgical intensive care units (ICUs) at a single academic institution between January 1, 2009, and December 31, 2013. Inclusion criteria included age ≥18 years and a platelet count measured during ICU admission. Propensity-matched analyses were used to evaluate associations between prophylactic platelet transfusions and the outcomes of interest with a primary outcome of red blood cell transfusion in the ensuing 24 hours and secondary outcomes of ICU and hospital-free days and changes in sequential organ failure assessment scores.
A total of 40,693 patients were included in the investigation with 3227 (7.9%) receiving a platelet transfusion and 1065 (33.0%) for which platelet transfusion was prophylactic in nature. In propensity-matched analyses, 994 patients with prophylactic platelet transfusion were matched to those without a transfusion. Patients receiving prophylactic platelets had significantly higher red blood cell transfusion rates (odds ratio 7.5 [5.9-9.5]; P < .001), fewer ICU-free days (mean [standard deviation] 20.8 [9.1] vs 22.7 [8.3] days; P = .004), fewer hospital-free days (13.0 [9.7] vs 15.8 [9.4] days; P < .001), and less improvement in sequential organ failure assessment scores (mean decrease of 0.2 [3.6] vs 1.8 [3.3]; P < .001) in the subsequent 24 hours. These findings appeared robust, persisting in multiple predefined sensitivity analyses.
Prophylactic administration of platelets in the critically ill was not associated with improved clinical outcomes, though residual confounding may exist. Further investigation of platelet transfusion strategies in this population is warranted.
血小板减少症在危重症患者中很常见,常预防性输注血小板以预防出血并发症。然而,这种做法的疗效尚不清楚。本研究的目的是确定危重症患者预防性血小板输注与出血并发症之间的关系。
这是一项回顾性队列研究,纳入了 2009 年 1 月 1 日至 2013 年 12 月 31 日期间在单一学术机构的外科、内科或内科-外科联合重症监护病房(ICU)住院的成年人。纳入标准包括年龄≥18 岁且 ICU 入院时测量血小板计数。采用倾向匹配分析评估预防性血小板输注与主要结局(随后 24 小时内输注红细胞)和次要结局(ICU 和住院无天数和序贯器官衰竭评估评分变化)之间的关联。
共纳入 40693 例患者,其中 3227 例(7.9%)接受血小板输注,1065 例(33.0%)为预防性输注血小板。在倾向匹配分析中,994 例接受预防性血小板输注的患者与未输注的患者相匹配。接受预防性血小板输注的患者红细胞输注率显著较高(比值比 7.5 [5.9-9.5];P <.001),ICU 无天数更少(平均[标准差]20.8 [9.1] vs 22.7 [8.3]天;P =.004),住院无天数更少(13.0 [9.7] vs 15.8 [9.4]天;P <.001),随后 24 小时序贯器官衰竭评估评分改善较少(平均下降 0.2 [3.6] vs 1.8 [3.3];P <.001)。这些发现似乎是稳健的,在多个预设的敏感性分析中仍然存在。
在危重症患者中预防性给予血小板并没有改善临床结局,但可能存在残留混杂因素。有必要进一步研究该人群中的血小板输注策略。